Visceral Fat: How to Measure and Reduce Metabolic Risk
Visceral fat is deep abdominal fat around internal organs, not the fat you can pinch. It matters because adipose tissue is endocrine and immune-active; excess visceral adiposity is linked with insulin resistance, high triglycerides, fatty liver, hypertension, type 2 diabetes, and cardiovascular risk. Start with waist circumference, waist-to-height ratio, blood pressure, labs, muscle, and fitness. Use DXA, MRI, or CT only when the result changes decisions.
Not cosmetic
Visceral fat is metabolically active adipose tissue, not just belly fat. The useful question is physiology, not appearance.
Use a hierarchy
MRI and CT measure directly, DXA can estimate, and most people should start with waist, waist-to-height ratio, labs, blood pressure, muscle, and fitness.
Aim for safer topology
The goal is not simply less weight. It is less visceral and ectopic metabolic stress while preserving muscle and cardiorespiratory fitness.
Before you scan
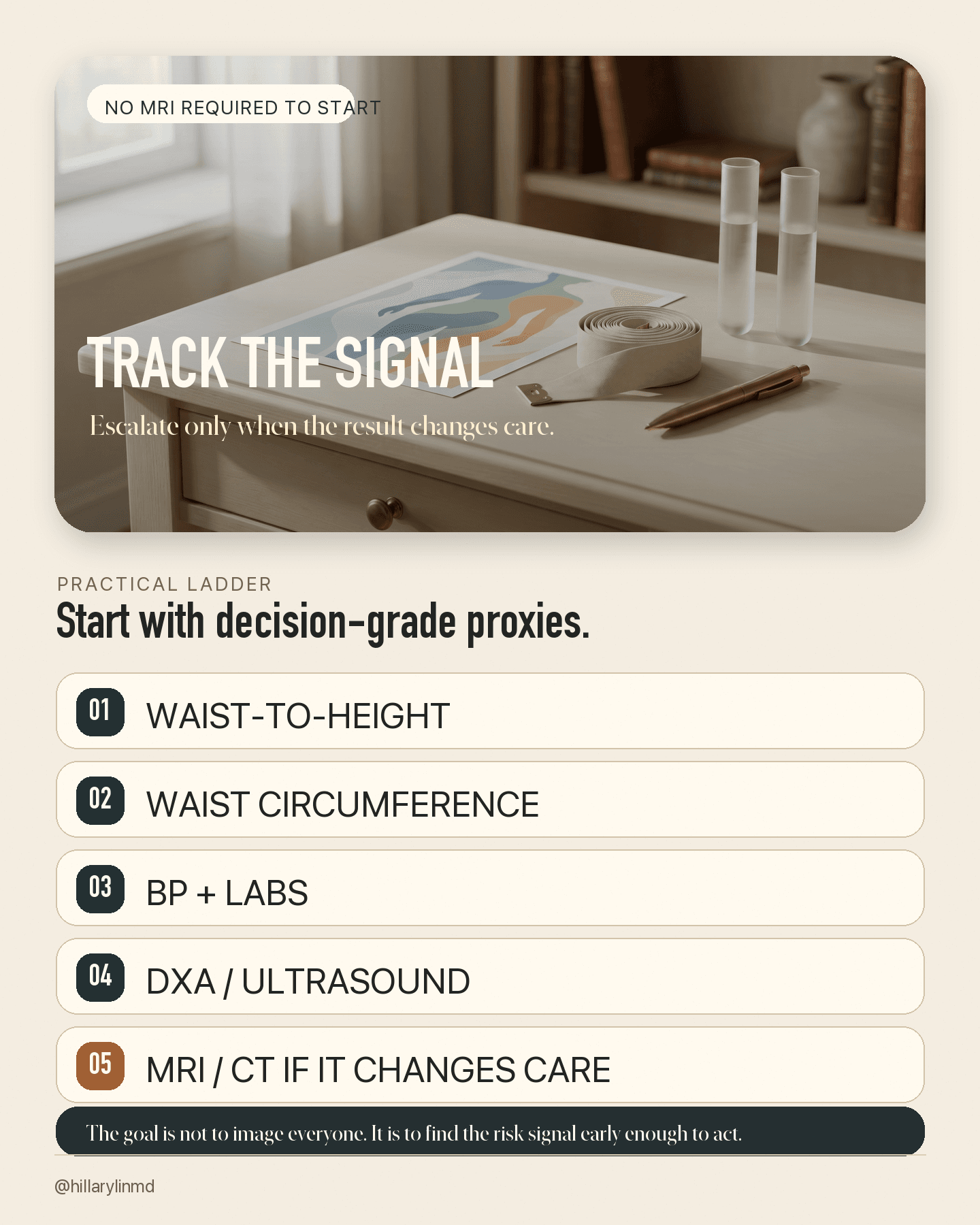
You do not need an MRI to start estimating visceral-fat risk at home.
Start with waist circumference, waist-to-height ratio, blood pressure, glucose or A1c, triglycerides and HDL, ApoB, liver markers, muscle, and fitness. Escalate to DXA or imaging only when the result would change management.
The short answer
Visceral fat is deep abdominal fat stored around internal organs. It is different from softer subcutaneous fat under the skin: the fat you can usually pinch.
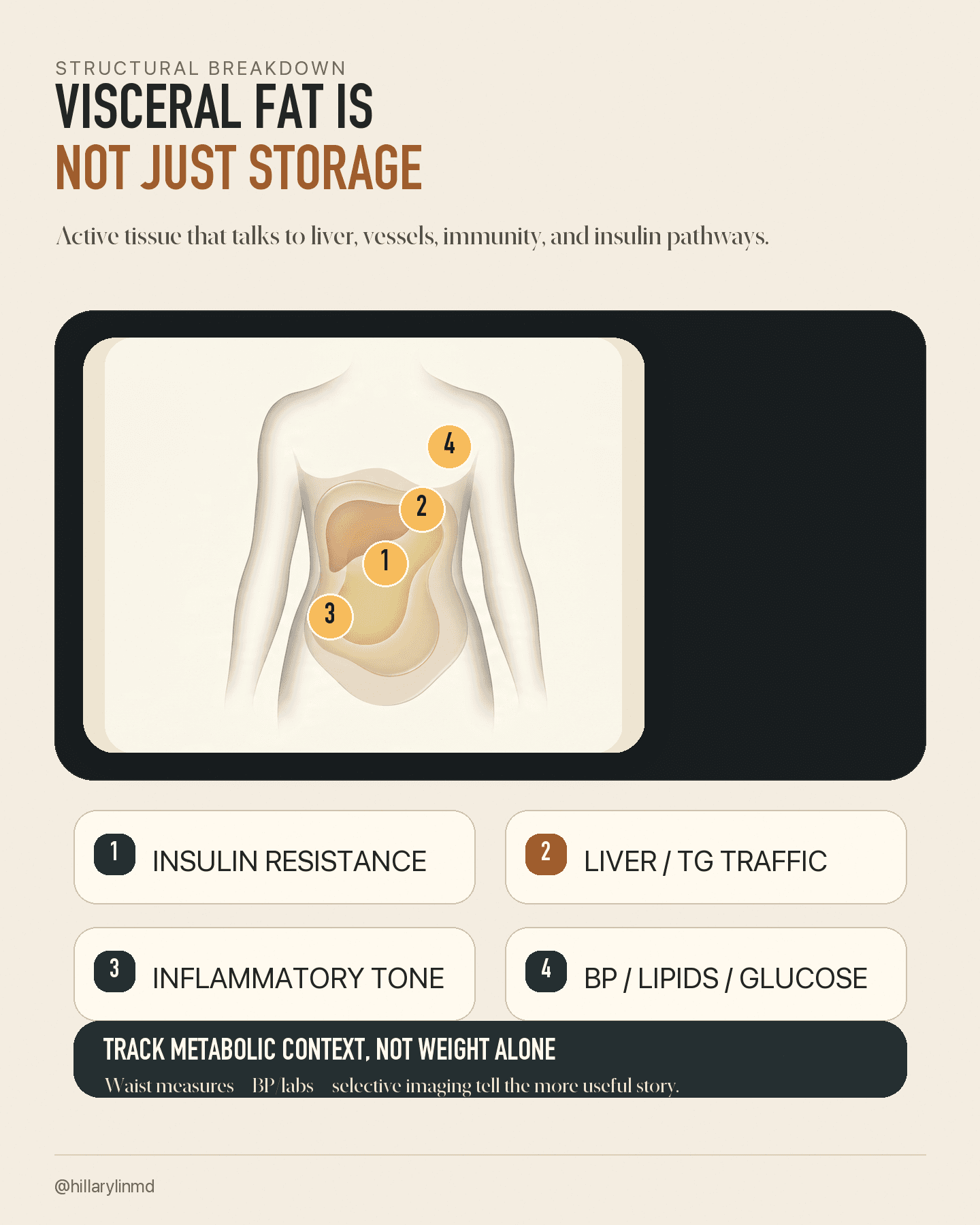
The reason visceral fat matters is not cosmetic. It is physiologic. Adipose tissue is an endocrine and immune-active organ. It secretes hormones, cytokines, inflammatory mediators, and metabolic signals. The visceral depot worries clinicians because it sits near internal organs, drains toward the liver, and is associated with insulin resistance, high triglycerides, fatty liver, hypertension, type 2 diabetes, and cardiovascular risk.
The scale can miss this. Two people can have the same BMI and very different visceral-fat burden, liver fat, muscle mass, glucose metabolism, and long-term risk. BMI tells me size. Visceral adiposity tells me physiology.
The practical takeaway: you do not need an MRI to start assessing visceral-fat risk. At home, waist circumference and waist-to-height ratio give useful proxy signals; routine vitals and labs add the context that makes the number actionable. MRI and CT can measure visceral fat directly. DXA can estimate distribution. Ultrasound and bioimpedance can provide rougher signals. Use the more advanced tests when the result would change the plan.
To reduce visceral-fat risk, the highest-yield levers are exercise dose, resistance training and muscle preservation, sustainable nutrition, sleep and apnea care, alcohol honesty, and clinical treatment of glucose, lipids, blood pressure, liver disease, PCOS, menopause-related changes, or obesity when relevant.
Useful frameadipose tissue is the organ you may not have thought to track; visceral fat is the depot that most changes the cardiometabolic story.
Safety framethis guide is educational, not individualized medical advice, and body-size metrics need extra care in pregnancy, eating-disorder recovery, complex illness, rapid weight change, or edema.
What visceral fat is
Body fat is not one uniform compartment. Subcutaneous fat sits under the skin. Visceral fat sits deep in the abdomen around organs, especially omental and mesenteric fat. Ectopic fat accumulates in places not designed to store much fat, such as liver, pancreas, skeletal muscle, heart, or around the heart.
Visceral fat is often called belly fat, but that phrase is imprecise. A visible abdomen can reflect subcutaneous fat, visceral fat, bloating, posture, muscle, anatomy, or normal body variation. The clinically relevant issue is not appearance. It is whether the body is storing energy in a depot that is metabolically disruptive.
A better definition: visceral fat is deep abdominal adipose tissue that can act as a metabolic risk amplifier, especially when it becomes inflamed, insulin-resistant, and linked to ectopic fat spillover.
Diagram
Three compartments, three meanings
The same body weight can hide very different storage patterns. The risk question is where energy is being stored and what signals that tissue is sending.
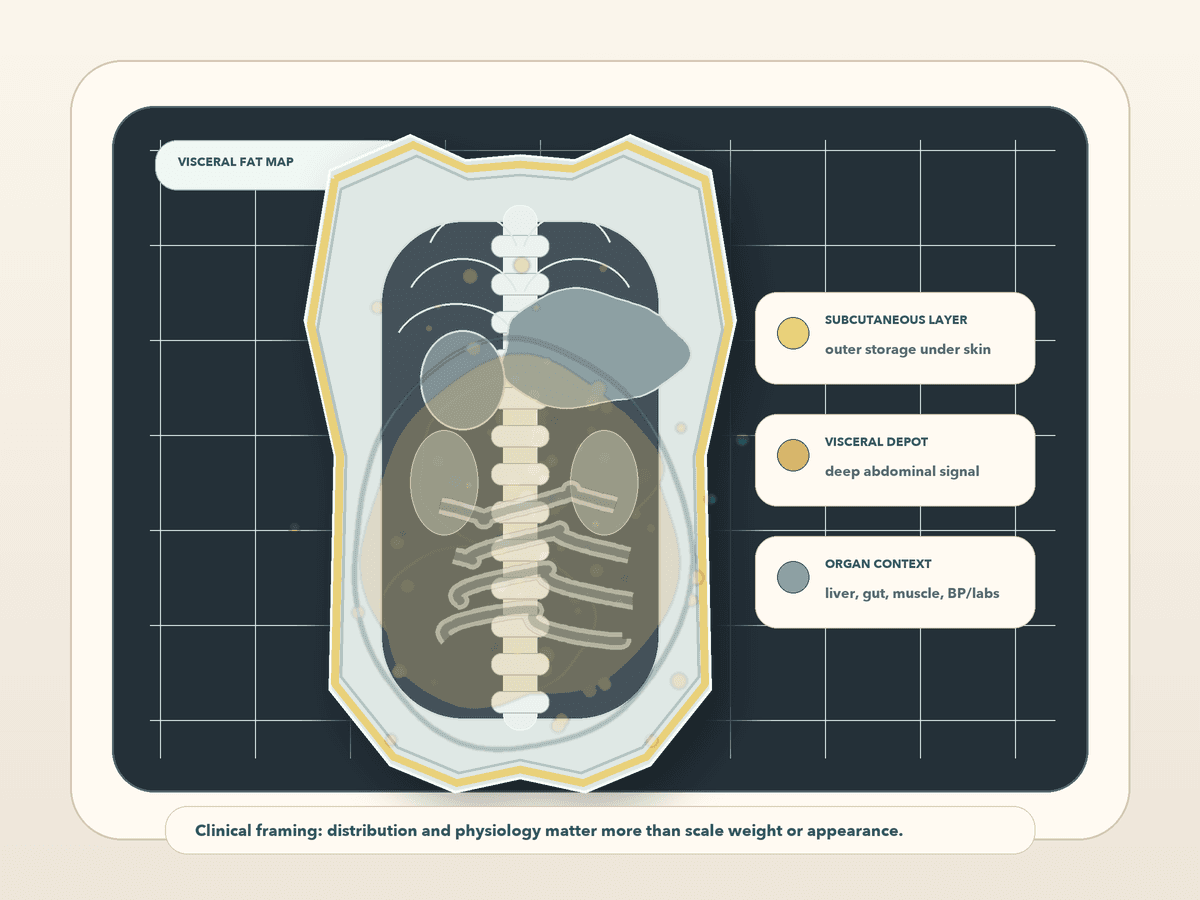
Subcutaneous
outer layerFat under the skin; often pinchable and sometimes a safer storage depot.
Not automatically benign or harmful. Location and metabolic context matter.
Visceral
deep depotDeep abdominal fat around organs; more tightly linked to insulin resistance, triglycerides, fatty liver, and diabetes risk.
This is the depot this guide focuses on.
Ectopic
spillover clueFat in liver, pancreas, muscle, or around the heart; a sign that storage has moved into higher-risk territory.
Often travels with visceral adiposity and metabolic dysfunction.
Why adipose tissue is an organ
It is tempting to think of fat as inert storage. That model is outdated. Adipose tissue secretes leptin, adiponectin, inflammatory cytokines, complement factors, coagulation-related signals, renin-angiotensin system components, and other mediators. These signals influence appetite, glucose handling, vascular biology, immune function, inflammation, and energy metabolism.
That is why adipose tissue is often described as an endocrine organ. This does not mean all fat is bad. A healthy subcutaneous depot can be protective because it gives the body a safer place to store energy. Problems arise when storage capacity is exceeded, visceral fat expands, adipose tissue becomes inflamed or fibrotic, and fat spills into liver, pancreas, muscle, or other ectopic locations.
Your fat is not luggage. It is signaling tissue.
Hidden organ map
Diagram
The visceral-fat risk pathway
A simplified way to explain why the depot matters more than the scale number alone.
Storage pressure
Energy storage demand rises or safer subcutaneous storage becomes insufficient.
Genetics, menopause, sleep, alcohol, inactivity, diet pattern, medication effects, and insulin resistance can all influence this.
Depot shift
More energy moves into visceral and ectopic compartments.
This is why waist and liver context can matter even when weight is stable.
Liver signal
Portal fatty-acid and inflammatory signaling can worsen hepatic insulin resistance and VLDL output.
The clinical pattern often includes triglycerides, glucose, BP, and fatty-liver clues.
Risk pattern
Central adiposity clusters with insulin resistance, hypertension, dyslipidemia, fatty liver, diabetes risk, and cardiovascular risk.
It is a risk architecture, not an aesthetic category.
Portal drainagemuch visceral fat drains toward the liver, which helps explain the link with liver insulin resistance, VLDL production, triglycerides, and glucose dysregulation.
Inflammatory remodelingunder metabolic stress, visceral adipose tissue can develop enlarged adipocytes, hypoxia, macrophage infiltration, fibrosis, and altered adipokine secretion.
Ectopic spilloverwhen safer storage is exceeded or dysfunctional, fat can accumulate in liver, pancreas, skeletal muscle, heart, and pericardial depots.
BMI limitationsome people carry high visceral or ectopic fat with a normal or only mildly elevated BMI, so size alone is not physiology.
What the long-term Circulation follow-up adds
A 2026 Circulation follow-up studied participants from two MRI-based lifestyle trials, CENTRAL and DIRECT-PLUS. These trials used dietary interventions, Mediterranean diet variants, and structured physical activity, with MRI measurements of visceral fat, subcutaneous fat, liver fat, pancreatic fat, and other depots.
Researchers followed participants 5 and 10 years after the original interventions. The useful finding was counterintuitive: participants regained weight, but some abdominal fat-depot improvements partially persisted.
The strongest content hook is that each 10% lifestyle-induced loss of visceral fat was associated with a 28% lower risk of incident type 2 diabetes during follow-up, with a hazard ratio of 0.72 and 95% confidence interval of 0.54 to 0.94. That is an association from the follow-up, not certainty for one individual.
Use this carefully. It does not prove that a 10% visceral-fat loss produces the same diabetes-risk change for every individual. But it does support a better prevention frame: the intervention target is not just weight loss. It is moving the risk tissue.
Evidence chart
Evidence map: what is strong, what is useful, what needs caution
Biology
Adipose tissue is endocrine and immune-active; visceral adipose tissue has distinct portal, inflammatory, and ectopic-fat links.
Strong reason to treat fat distribution as physiology, not cosmetics.
Imaging cohorts
CT and MRI cohorts link visceral fat more strongly than subcutaneous fat to cardiometabolic risk factors and incident diabetes patterns.
Supports looking beyond BMI and total body fat.
Waist consensus
Waist circumference adds risk information beyond BMI and has been proposed as a clinical vital sign.
Best low-cost first-line proxy for central adiposity trend.
Lifestyle VAT loss
MRI-based lifestyle trials show visceral-fat reductions can occur with diet and exercise, and the 2026 follow-up links intervention-induced VAT loss with lower diabetes incidence.
Strong prevention signal, but not a personal prediction for one person.
Measurement devices
DXA, ultrasound, and BIA can estimate or proxy visceral fat with variable accuracy versus MRI/CT.
Use for trends and decisions only when the method is reliable enough for the question.
Evidence hierarchy: direct imaging and longitudinal clinical outcomes carry more weight than a proprietary smart-scale score.
How to measure visceral fat without losing the plot
There are four useful levels of measurement: direct imaging, body-composition estimates, anthropometric proxies, and metabolic clues. The higher-tech number is not automatically the better decision tool.
MRI and CT are reference methods for measuring visceral and subcutaneous abdominal fat compartments. MRI avoids radiation and can quantify multiple fat depots if the protocol supports it. CT is reproducible and widely used in research, but radiation makes it a poor routine tracking tool for curiosity. A single CT or MRI slice can approximate visceral-fat volume in some protocols, but it is not identical to full volumetric segmentation.
DXA body-composition scans can estimate visceral fat in the android abdominal region and can be useful when lean mass, fat mass, bone, or a rough VAT estimate will change decisions. Ultrasound can estimate visceral or preperitoneal fat depth, but it is operator- and protocol-dependent. BIA, InBody-style devices, and smart scales can be useful for engagement or trend awareness, but they are not diagnostic.
For most people, waist circumference and waist-to-height ratio are the practical starting point. NICE uses a public-facing message of keeping waist less than half of height, or a waist-to-height ratio under 0.5, while recognizing context and limitations.
Tracking hierarchy
Protocol
Measurement stack: direct tests, estimates, and practical proxies
MRI
- What it tells you
- Direct no-radiation quantification of visceral, subcutaneous, and sometimes ectopic fat depending on protocol.
- How to use it
- Best reference option when the result will change management; expensive and protocol-dependent.
CT
- What it tells you
- Direct and reproducible abdominal fat measurement.
- How to use it
- Useful clinically when already indicated or in research; not a routine tracking tool because of radiation.
DXA
- What it tells you
- Body composition plus an estimated android-region visceral-fat value in some systems.
- How to use it
- Useful for lean mass, fat mass, bone, and VAT trend if the algorithm and conditions are consistent.
Ultrasound
- What it tells you
- Radiation-free estimate of visceral or preperitoneal fat depth.
- How to use it
- Promising, but operator and protocol matter.
BIA / smart scale
- What it tells you
- Algorithmic estimate or visceral-fat level influenced by hydration, meals, exercise, temperature, and device model.
- How to use it
- Trend or engagement signal only. A smart scale can start the conversation; it should not end it.
Waist and waist-to-height
- What it tells you
- Low-cost proxy for central adiposity and risk trend.
- How to use it
- Best practical default: standardize method, measure monthly, and interpret with labs, BP, muscle, and fitness.
Labs and fitness
- What it tells you
- Glucose, A1c, triglycerides/HDL, ApoB, BP, liver signals, muscle, and VO2 context.
- How to use it
- Do not diagnose visceral fat, but clustered changes raise suspicion and guide the plan.
| Level | What it tells you | How to use it |
|---|---|---|
| MRI | Direct no-radiation quantification of visceral, subcutaneous, and sometimes ectopic fat depending on protocol. | Best reference option when the result will change management; expensive and protocol-dependent. |
| CT | Direct and reproducible abdominal fat measurement. | Useful clinically when already indicated or in research; not a routine tracking tool because of radiation. |
| DXA | Body composition plus an estimated android-region visceral-fat value in some systems. | Useful for lean mass, fat mass, bone, and VAT trend if the algorithm and conditions are consistent. |
| Ultrasound | Radiation-free estimate of visceral or preperitoneal fat depth. | Promising, but operator and protocol matter. |
| BIA / smart scale | Algorithmic estimate or visceral-fat level influenced by hydration, meals, exercise, temperature, and device model. | Trend or engagement signal only. A smart scale can start the conversation; it should not end it. |
| Waist and waist-to-height | Low-cost proxy for central adiposity and risk trend. | Best practical default: standardize method, measure monthly, and interpret with labs, BP, muscle, and fitness. |
| Labs and fitness | Glucose, A1c, triglycerides/HDL, ApoB, BP, liver signals, muscle, and VO2 context. | Do not diagnose visceral fat, but clustered changes raise suspicion and guide the plan. |
For longitudinal tracking, consistency matters: same modality, anatomical level, software, protocol, device, and conditions.
Waist methodmeasure midway between the bottom of the ribs and the top of the hip bone after a normal exhale, with the tape level and snug but not compressing skin.
Trend rulemonthly is enough for most people. Weekly measurement can create noise and body surveillance.
Clinical clueif weight is stable but waist is rising, the story changed.
How to reduce visceral fat without losing muscle
If the question is how to reduce visceral fat, the answer is not a cleanse or a spot-exercise plan. The evidence is strongest for lifestyle interventions that combine nutrition, physical activity, muscle preservation, and cardiometabolic risk management. Exercise is one of the most important tools because it can reduce visceral fat even when scale change is modest.
Aerobic exercise, moderate-to-vigorous exercise, and HIIT have all shown visceral-fat reduction in randomized trials and meta-analyses. Resistance training matters too, especially because preserving muscle changes the risk equation. The goal is not simply to weigh less; it is to reduce visceral and ectopic fat while maintaining or increasing lean mass and fitness.
Nutrition still matters, but not as a purity contest. Caloric balance, Mediterranean-style patterns, higher fiber, adequate protein, less ultra-processed food, improved alcohol patterns, and reduced refined-carbohydrate load can all be useful depending on the person. The useful plan is the one someone can sustain while improving cardiometabolic markers and preserving muscle.
Medical context matters too. Type 2 diabetes, PCOS, menopause transition, MASLD, hypothyroidism, Cushing physiology, medication effects, sleep apnea, and obesity requiring medical treatment can all change the plan. The point is not to self-prescribe. The point is to recognize that visceral adiposity is often part of a clinical pattern, not a willpower problem.
Stack chart
Intervention stack: what moves the risk pattern
Aerobic work
Regular Zone 2 / moderate aerobic volume with progression.
Improves glucose disposal, mitochondrial capacity, blood pressure, triglycerides, and visceral-fat biology.
Intensity
Moderate-to-vigorous exercise or HIIT when recovery and risk allow.
Can reduce VAT efficiently, but should not outrun sleep, joints, BP, or symptoms.
Strength
Two to three resistance sessions weekly when feasible.
Preserves lean mass so weight loss does not become muscle loss.
Nutrition
Protein, fiber, Mediterranean-style pattern, less ultra-processed food, alcohol honesty, and a sustainable energy deficit when appropriate.
Targets central adiposity without turning the plan into punishment.
Sleep / apnea / stress
Treat sleep apnea, improve sleep regularity, reduce alcohol where relevant, and lower chronic stress load.
These influence glucose regulation, appetite signaling, BP, and fat distribution.
Medical care
Treat diabetes, MASLD, PCOS, menopause-related changes, hypertension, dyslipidemia, and medication contributors when present.
The visceral-fat pattern often needs clinical risk management, not just lifestyle slogans.
The goal is not a smaller body. The goal is a safer metabolic topology.
What I would track in practice
If someone asked me how to monitor visceral-fat risk without obsessing over body size, I would use a hierarchy. Start with the measures that are cheap, repeatable, and tied to decisions. Escalate to imaging only when it changes the plan.
If weight is falling but muscle is falling faster than fat, the story is not automatically good. If waist is falling, triglycerides are improving, BP is improving, glucose is improving, and strength is preserved, that may be a win even when the scale is being emotionally unhelpful.
1. Waist circumference monthly, standardized and unemotional.
2. Waist-to-height ratio, especially when BMI is not telling the full story.
3. Blood pressure, ideally clean home averages if elevated.
4. Glucose metabolismfasting glucose, A1c, sometimes fasting insulin or CGM context.
5. Lipidstriglycerides/HDL pattern and ApoB.
6. Liver signalsALT, GGT, fatty-liver context, and imaging if clinically indicated.
7. Body compositionDXA only when accessible and management-changing, not as a body-surveillance metric.
8. Muscle and fitnessstrength, lean mass, VO2/cardiorespiratory fitness, and weekly exercise dose.
Common mistakes and cautions
The point of tracking visceral-fat risk is better context, not body surveillance. These are the mistakes I see most often when people discover the metric.
Decision matrix
Benefit and caution map
BMI is normal but waist and triglycerides are rising
Look beyond size and check central adiposity, glucose, BP, liver, muscle, and fitness context.Do not assume appearance rules risk in or out.
Smart scale reports high visceral fat
Use it as a reason to standardize waist and review labs or BP.Do not treat one proprietary number as a diagnosis.
DXA estimates VAT
Helpful if it sits inside a broader body-composition and muscle-preservation plan.DXA VAT is an estimate, not the same as MRI or CT segmentation.
Weight loss is fast
Check whether waist, BP, glucose, triglycerides, and liver markers are improving.Protect muscle with protein, resistance training, and adequate recovery.
Waist tracking feels psychologically loaded
Use clinician-guided labs, BP, fitness, and body-composition context instead.A metric that worsens health is not a good metric for that person.
Curiosity scan
Can be useful for a high-end baseline if the person understands limits.MRI is not the default; CT is not for routine curiosity because of radiation.
This is physiology, not shame. The tape measure is not an aesthetic tool here. It is a risk-topology tool.
Hillary’s take
Visceral fat is one of the cleanest examples of why weight is an incomplete health metric. The scale can tell you whether mass changed. It cannot tell you whether the intervention moved energy out of the wrong compartment, protected muscle, improved liver fat, lowered triglycerides, improved insulin sensitivity, or reduced blood pressure.
I do not want people to obsess over scans or turn waist circumference into another shame metric. I want the opposite: better context, less false precision, and fewer people being reassured or discouraged by the wrong number.
The goal is not a smaller body. The goal is a safer metabolic topology.
Clinical lens
How I’d decide
Use this section as a second pass after the main answer, not as homework before you know what the page is saying.
Who it’s for
Adults who want a better cardiometabolic-risk signal than weight alone, especially if waist is rising, triglycerides or glucose are drifting, blood pressure is increasing, fatty liver or MASLD is present, menopause or PCOS is changing body composition, or family history makes diabetes prevention a priority.
Who should skip it
Do not turn this into self-scoring if you are pregnant or postpartum, in eating-disorder recovery, dealing with rapid unexplained weight change, edema, cancer treatment, complex illness, major medication changes, or body-size surveillance that worsens health. Use clinician context instead.
Measure before / after
Start with monthly waist circumference, waist-to-height ratio, blood pressure, glucose or A1c context, triglycerides and HDL, ApoB when appropriate, liver markers or fatty-liver context, muscle and strength, and cardiorespiratory fitness. DXA, ultrasound, MRI, or CT are useful only when the result will change decisions.
What I’d do first
I would begin with a standardized waist trend plus cardiometabolic labs, then build the plan around aerobic exercise, resistance training, protein and fiber adequacy, sustainable nutrition, sleep and apnea risk, alcohol honesty, blood pressure, glucose, lipids, liver risk, and muscle preservation.
What would change my mind
I would escalate from proxy tracking to imaging when the result changes risk communication, clinical management, medication strategy, research enrollment, or a high-stakes baseline. I would de-emphasize a body-composition number if it worsens obsession, ignores muscle, or distracts from blood pressure, glucose, lipids, liver risk, sleep, and fitness.
Frequently Asked Questions
Is visceral fat the same as belly fat?
Not exactly. Belly fat is a visual phrase. It can include subcutaneous fat under the skin and visceral fat deep around organs. Visceral fat is the metabolically higher-risk depot, but appearance alone cannot reliably identify it.
Can thin people have visceral fat?
Yes. Some people with normal BMI can carry disproportionate visceral or ectopic fat and show insulin resistance, fatty liver, high triglycerides, or central adiposity. This is why waist, labs, blood pressure, and fitness context matter.
What is the best way to measure visceral fat?
MRI and CT are the reference methods. MRI avoids radiation; CT is reproducible but uses ionizing radiation. DXA can estimate visceral fat and is more accessible in some settings. Most people do not need direct imaging unless it changes management.
Are InBody or smart-scale visceral-fat scores accurate?
They can be useful as rough trend signals, but they are not diagnostic. Hydration, recent food, exercise, temperature, device algorithms, and measurement conditions matter. Use the same device under similar conditions and interpret cautiously.
What waist-to-height ratio should I aim for?
NICE uses a practical public message: try to keep waist less than half of height, or a waist-to-height ratio under 0.5. This is a screening tool, not a universal diagnosis. Context matters, especially in pregnancy or postpartum, high muscle mass, illness, eating-disorder history, and different body types.
Can exercise reduce visceral fat without major weight loss?
Yes. Exercise can reduce visceral fat even when scale-weight change is modest. This is one reason exercise should not be reduced to calorie burning. It changes fat-depot biology, insulin sensitivity, muscle, fitness, blood pressure, and triglycerides.
Does losing visceral fat lower diabetes risk?
A 2026 Circulation follow-up of lifestyle-intervention trials found that each 10% intervention-induced visceral-fat loss was associated with a 28% lower risk of incident type 2 diabetes over follow-up. This supports visceral-fat loss as a meaningful target, but it should be read as association, not personal certainty.
Is subcutaneous fat bad?
Not necessarily. Subcutaneous fat can be a safer energy-storage depot, and lower-body or gluteofemoral fat may be metabolically protective in some contexts. The goal is not no fat. The goal is healthier storage and less visceral or ectopic metabolic stress.
How often should I measure waist circumference?
Monthly is enough for most people. Weekly measurements can create noise and body surveillance. Use a standardized method and track the trend rather than reacting to one reading.
How do you reduce visceral fat?
Reduce visceral fat by starting with the basics that move physiology: consistent aerobic exercise, resistance training, adequate protein, fiber, a sustainable nutrition pattern, less ultra-processed food and alcohol where relevant, sleep quality, blood-pressure control, glucose, lipid, and liver-marker monitoring, and clinical care for diabetes, fatty liver, PCOS, menopause-related changes, sleep apnea, or obesity when present.
References & citations
- 1.Ahima RS, Flier JS. Adipose tissue as an endocrine organ. Trends Endocrinol Metab, 2000
- 2.Kershaw EE, Flier JS. Adipose tissue as an endocrine organ. J Clin Endocrinol Metab, 2004
- 3.Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update. Physiol Rev, 2013
- 4.Lee MJ, Kim J. The pathophysiology of visceral adipose tissues in cardiometabolic diseases. Biochem Pharmacol, 2024
- 5.Fox CS, Massaro JM, Hoffmann U, et al. Abdominal visceral and subcutaneous adipose tissue compartments. Circulation, 2007
- 6.Neeland IJ, Turer AT, Ayers CR, et al. Dysfunctional adiposity and risk of prediabetes and type 2 diabetes. JAMA, 2012
- 7.Britton KA, Massaro JM, Murabito JM, et al. Body fat distribution, incident cardiovascular disease, cancer, and mortality. JACC, 2013
- 8.Chandra A, Neeland IJ, Berry JD, et al. Body mass, fat distribution, and incident hypertension. JACC, 2014
- 9.Kammerlander AA, Lyass A, Mahoney TF, et al. Sex differences in visceral adipose tissue associations. JAHA, 2021
- 10.Ross R, Neeland IJ, Yamashita S, et al. Waist circumference as a vital sign in clinical practice. Nat Rev Endocrinol, 2020
- 11.Murphy J, Bacon SL, Morais JA, et al. Intra-abdominal adipose tissue quantification by alternative versus reference methods. Obesity, 2019
- 12.Kaul S, Rothney MP, Peters DM, et al. Dual-energy X-ray absorptiometry for quantification of visceral fat. Obesity, 2012
- 13.Savva SC, Lamnisos D, Kafatos AG. Waist-to-height ratio or BMI for cardiometabolic risk: meta-analysis. Diabetes Metab Syndr Obes, 2013
- 14.NICE. Overweight and obesity management: identifying and assessing overweight, obesity and central adiposity. NG246
- 15.Gepner Y, Shelef I, Schwarzfuchs D, et al. Effect of distinct lifestyle interventions on mobilization of fat storage pools. Circulation, 2018
- 16.Klein H, Alufer L, Goldberg Toren DT, et al. Lifestyle-induced visceral fat loss as a key target for durable cardiometabolic health. Circulation, 2026
- 17.Vissers D, Hens W, Taeymans J, et al. The effect of exercise on visceral adipose tissue in overweight adults. PLoS One, 2013
Related Guides
Metabolic risk hierarchy
Use the guide to choose the next measurement, not the fanciest one.
Visceral fat is useful only when it changes decisions: waist trend, labs, blood pressure, liver risk, muscle, fitness, and selective body-composition testing when the result will actually change the plan.