How to Prevent Atherosclerosis: A First-Principles Guide to Lipids and Plaque
Preventing atherosclerosis means lowering cumulative ApoB particle exposure and controlling the forces that injure the artery wall. I would start with a standard lipid panel plus ApoB and one-time Lp(a), blood pressure, metabolic risks, kidney function, smoking, and family history, then use CAC or CCTA selectively only when the result changes treatment.
Think in particle-years
ApoB-containing particles cause atherosclerosis through cumulative exposure. A moderately high burden for decades can matter more than one dramatic lab result.
Separate the layers
ApoB, Lp(a), blood pressure, metabolic health, CAC, CCTA, and stress testing answer different questions. No single marker replaces the rest.
Use the lightest durable plan
Start with lifestyle and the lowest-burden therapy likely to reach the needed reduction, then escalate based on risk, response, evidence, tolerance, and adherence.
Atherosclerosis is a particle, wall, terrain, plaque, and clot problem
Heart disease changed my family long before it changed my lab work. My father survived a massive heart attack and ultimately needed a heart transplant. My grandfather spent the last six years of his life bed-bound after a stroke. Then my own untreated LDL-C came back at 192 mg/dL. That is why I do not think about prevention as a one-time cholesterol test. I think about the exposure an artery experiences over decades.
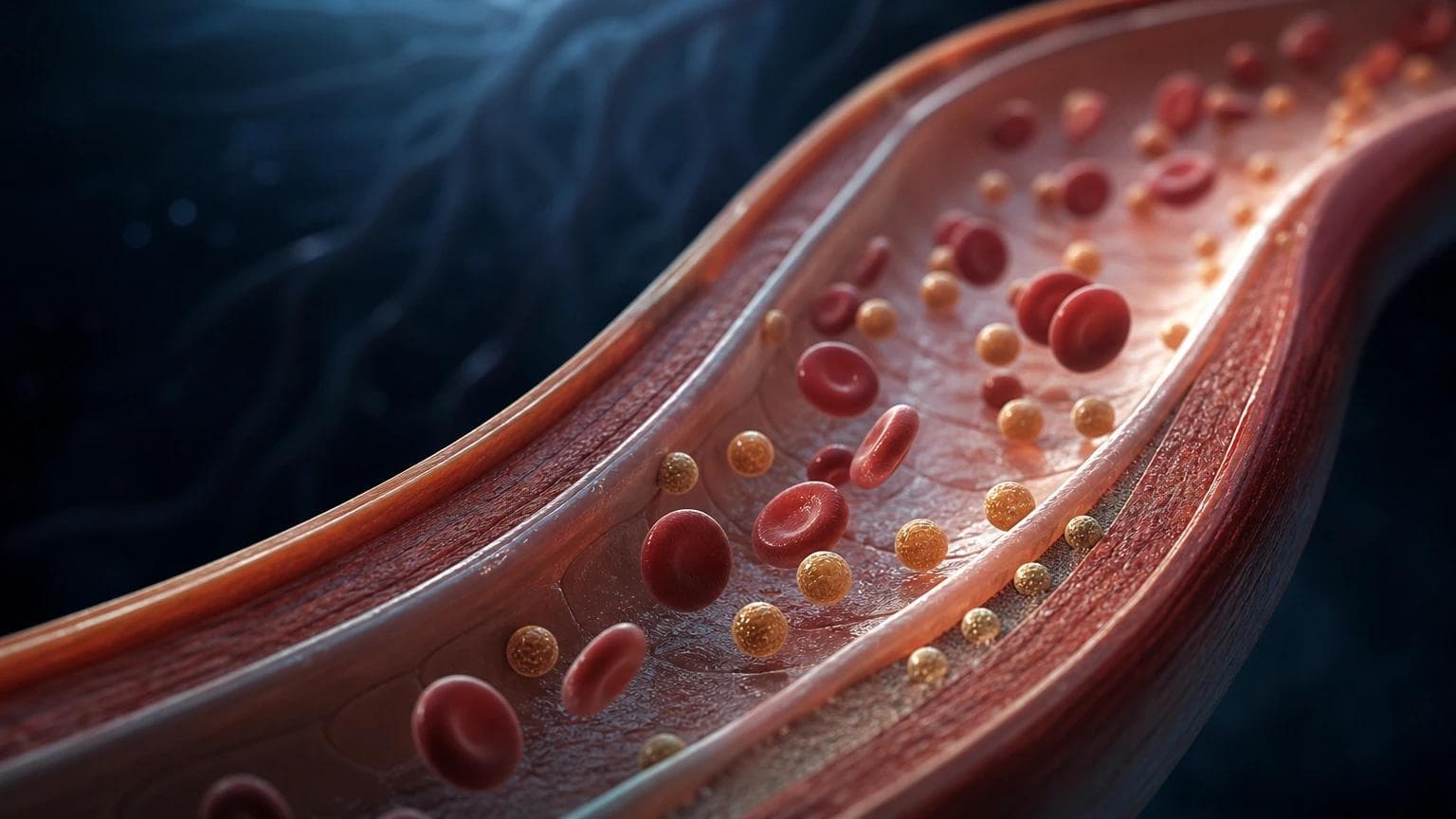
Atherosclerosis begins when ApoB-containing particles enter and become retained in the artery wall. LDL is the best-known particle, but remnants, IDL, and lipoprotein(a), or Lp(a), also carry ApoB. Retention triggers a local response involving endothelial dysfunction, oxidation, macrophages, foam cells, smooth-muscle remodeling, a fibrous cap, calcification, and sometimes plaque rupture or erosion followed by a clot.
The practical model is particles, wall, terrain, plaque, and clot. ApoB estimates the number of atherogenic particles. Blood pressure, smoking, diabetes, kidney disease, sleep apnea, inflammatory disease, and metabolic dysfunction shape the terrain and mechanical force. CAC and CCTA show different forms of visible disease. Thrombosis turns a stable burden into an acute event. Good prevention addresses the whole model without pretending every layer is equally measurable or equally causal.
Interactive artery-wall story
Plaque is a continuum, not a switch
Follow one active step at a time. The biology starts with retained ApoB particles and can end with thrombosis, but the path is dynamic rather than inevitable.
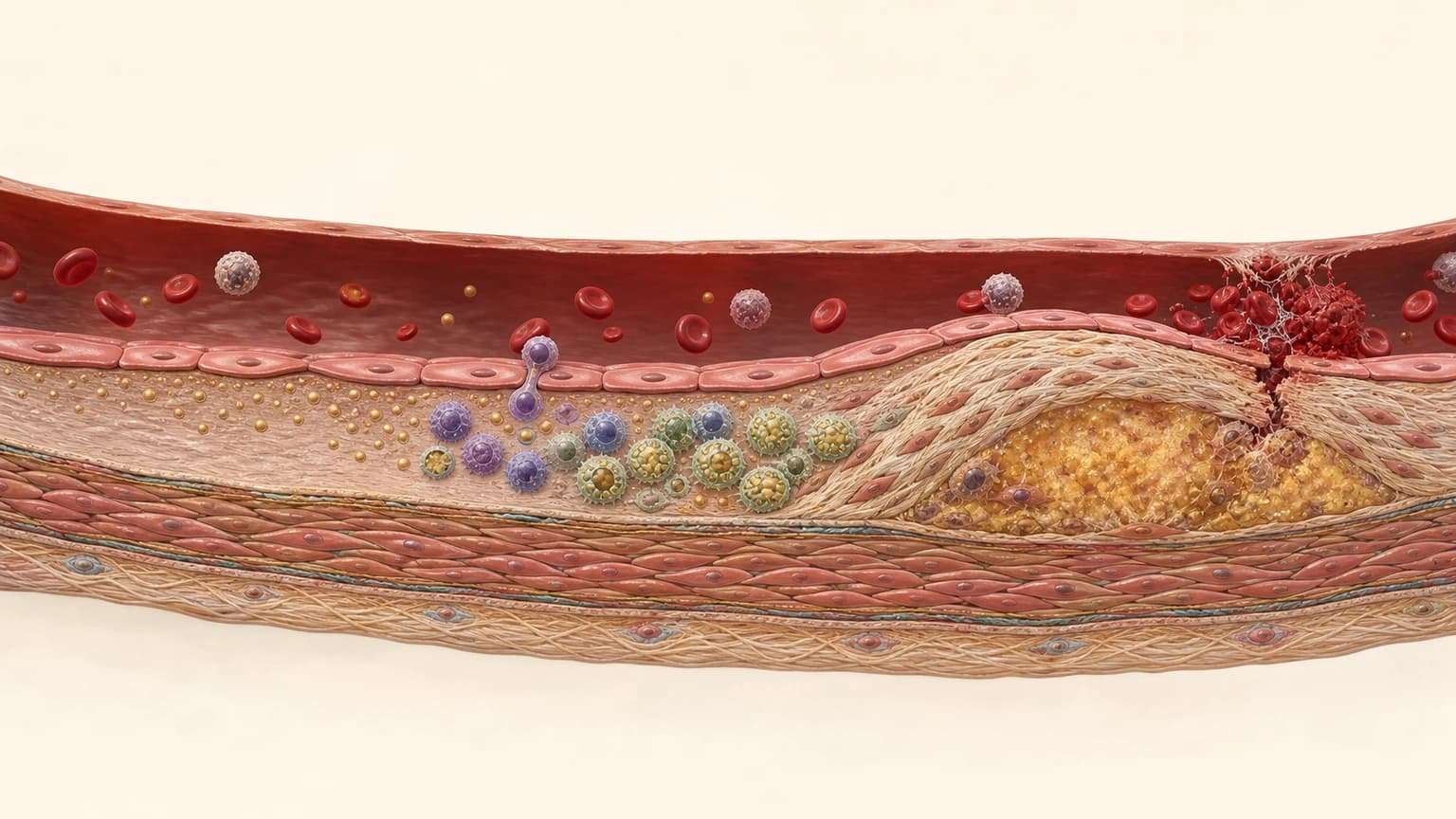
Simplified teaching model: real plaques can progress, stabilize, calcify, erode, rupture, or remodel in overlapping ways.
Diagram
The five-layer atherosclerosis model
Use the model to decide what each test or intervention is actually answering.
Particles
ApoB-containing LDL, remnants, IDL, and Lp(a) circulate and can enter the artery wall.
Primary measurement: ApoB, supported by LDL-C and non-HDL-C.
Wall
Endothelium, particle retention, inflammation, macrophages, smooth muscle, and fibrous-cap biology determine what happens after entry.
This biology is real, but no routine blood test fully summarizes it.
Terrain and force
Blood pressure, smoking, diabetes, kidney disease, sleep apnea, metabolic dysfunction, and inflammatory disease accelerate injury.
These can amplify risk even when a lipid panel looks acceptable.
Plaque
CAC, CCTA, and carotid imaging reveal different aspects of disease burden and composition.
A normal test only answers the question that test can see.
Clot and event
Plaque rupture or erosion plus thrombosis can produce myocardial infarction or ischemic stroke.
Event risk is not identical to cholesterol level or plaque volume alone.
Favorable metabolism helpsLow triglycerides, normal glucose, fitness, and low inflammation improve the terrain.
Favorable metabolism does not erase ApoBA clean metabolic profile cannot make decades of high particle exposure biologically irrelevant.
Visible plaque changes urgencyOnce plaque is present, the conversation shifts from predicting disease to slowing progression and preventing events.
Start with the measurements that change decisions
I want enough data to identify particle burden, inherited risk, major accelerants, and existing disease. I do not want a giant laboratory menu that creates more noise than action. For most prevention-minded adults, the useful baseline is a standard lipid panel, non-HDL-C, ApoB, Lp(a) at least once, blood pressure, glucose or A1c, kidney function, smoking status, medication review, and a careful family history.
LDL-C and ApoB are related but not interchangeable. LDL-C estimates the amount of cholesterol carried inside LDL particles. ApoB is closer to a count of all atherogenic particles because each LDL, VLDL remnant, IDL, and Lp(a) particle carries one ApoB molecule. When ApoB and LDL-C disagree, risk often tracks more closely with ApoB, especially with insulin resistance, high triglycerides, diabetes, obesity, and treated lipid states.
Lp(a) is different again. It is a genetically determined ApoB-containing particle with additional proatherogenic, inflammatory, oxidized-phospholipid, and aortic-valve relevance. Lifestyle usually does not lower it meaningfully. The 2026 ACC/AHA guideline recommends measuring it at least once in adulthood.
Protocol
What each measurement answers
LDL-C
- What it tells you
- Cholesterol mass carried inside LDL particles
- Where it changes the plan
- Guideline goals, treatment response, and the evidence base for LDL-lowering therapy
Non-HDL-C
- What it tells you
- Cholesterol carried by all ApoB-containing particles
- Where it changes the plan
- A no-extra-cost secondary target, particularly useful when triglycerides are elevated
ApoB
- What it tells you
- Concentration of atherogenic particles
- Where it changes the plan
- Discordant LDL-C, metabolic disease, high triglycerides, low achieved LDL-C, and residual risk
Lp(a)
- What it tells you
- Inherited Lp(a) particle burden
- Where it changes the plan
- Earlier or more intensive control of modifiable risk, family testing, and selected specialist or imaging decisions
Triglycerides
- What it tells you
- Remnant-rich metabolism and, when very high, pancreatitis risk
- Where it changes the plan
- Diet, alcohol, diabetes, weight, secondary causes, and targeted therapy in selected risk states
Blood pressure, A1c/glucose, eGFR, urine albumin
- What it tells you
- Artery-wall force and cardiometabolic or kidney accelerants
- Where it changes the plan
- Treatment urgency and the non-lipid prevention plan
Family history and prior pregnancy history
- What it tells you
- Lifetime risk that a 10-year calculator can miss
- Where it changes the plan
- Earlier testing, possible familial hypercholesterolemia workup, and lower threshold to treat
| Measurement | What it tells you | Where it changes the plan |
|---|---|---|
| LDL-C | Cholesterol mass carried inside LDL particles | Guideline goals, treatment response, and the evidence base for LDL-lowering therapy |
| Non-HDL-C | Cholesterol carried by all ApoB-containing particles | A no-extra-cost secondary target, particularly useful when triglycerides are elevated |
| ApoB | Concentration of atherogenic particles | Discordant LDL-C, metabolic disease, high triglycerides, low achieved LDL-C, and residual risk |
| Lp(a) | Inherited Lp(a) particle burden | Earlier or more intensive control of modifiable risk, family testing, and selected specialist or imaging decisions |
| Triglycerides | Remnant-rich metabolism and, when very high, pancreatitis risk | Diet, alcohol, diabetes, weight, secondary causes, and targeted therapy in selected risk states |
| Blood pressure, A1c/glucose, eGFR, urine albumin | Artery-wall force and cardiometabolic or kidney accelerants | Treatment urgency and the non-lipid prevention plan |
| Family history and prior pregnancy history | Lifetime risk that a 10-year calculator can miss | Earlier testing, possible familial hypercholesterolemia workup, and lower threshold to treat |
Advanced particle-size and fractionation panels can add nuance in selected cases, but they usually do not replace a standard lipid panel plus ApoB and Lp(a).
When the results disagree, ask which layer each result can see
Discordant results are common. The mistake is forcing them into one winner. A high ApoB and a CAC score of zero are not contradictory. One measures current particle burden; the other shows no detectable calcified coronary plaque at that moment. A high Lp(a) with a low ApoB is also not a reason to ignore Lp(a). Lp(a) carries independent inherited risk, while ApoB still helps quantify the modifiable particle burden around it.
I use disagreement to sharpen the question. Is the standard lipid panel undercounting particle risk? Is a low near-term plaque signal being mistaken for low lifetime risk? Has disease already appeared despite unremarkable current labs? Does inherited risk justify treating modifiable exposure more aggressively?
Protocol
Decision matrix: common discordant patterns
LDL-C looks acceptable, ApoB is high
- What it may mean
- More atherogenic particles than the cholesterol mass suggests
- What I would clarify next
- Triglycerides, insulin resistance, remnants, treatment response, and total-risk context
ApoB is high, CAC is zero
- What it may mean
- Current particle exposure with no detectable calcified coronary plaque
- What I would clarify next
- Age, duration of exposure, Lp(a), family history, FH, and whether a result would change treatment
CAC is positive, current lipids are modest
- What it may mean
- Atherosclerotic disease is already present even if today's lab values are not dramatic
- What I would clarify next
- Prior untreated exposure, blood pressure, smoking, diabetes, kidney risk, and treatment intensity
Lp(a) is high, other markers look good
- What it may mean
- An inherited risk enhancer that lifestyle rarely lowers directly
- What I would clarify next
- Compress ApoB/LDL-C and every modifiable risk factor; consider family testing and specialist input
Triglycerides are high, LDL-C is normal
- What it may mean
- Remnant-rich or insulin-resistant physiology may be hiding particle burden
- What I would clarify next
- ApoB, non-HDL-C, glucose control, alcohol, diet, thyroid, medications, and pancreatitis risk if severe
Stress test is normal, CCTA shows plaque
- What it may mean
- No inducible ischemia does not mean no atherosclerosis
- What I would clarify next
- Treat plaque burden and risk factors; use symptoms and anatomy to guide further cardiology evaluation
| Pattern | What it may mean | What I would clarify next |
|---|---|---|
| LDL-C looks acceptable, ApoB is high | More atherogenic particles than the cholesterol mass suggests | Triglycerides, insulin resistance, remnants, treatment response, and total-risk context |
| ApoB is high, CAC is zero | Current particle exposure with no detectable calcified coronary plaque | Age, duration of exposure, Lp(a), family history, FH, and whether a result would change treatment |
| CAC is positive, current lipids are modest | Atherosclerotic disease is already present even if today's lab values are not dramatic | Prior untreated exposure, blood pressure, smoking, diabetes, kidney risk, and treatment intensity |
| Lp(a) is high, other markers look good | An inherited risk enhancer that lifestyle rarely lowers directly | Compress ApoB/LDL-C and every modifiable risk factor; consider family testing and specialist input |
| Triglycerides are high, LDL-C is normal | Remnant-rich or insulin-resistant physiology may be hiding particle burden | ApoB, non-HDL-C, glucose control, alcohol, diet, thyroid, medications, and pancreatitis risk if severe |
| Stress test is normal, CCTA shows plaque | No inducible ischemia does not mean no atherosclerosis | Treat plaque burden and risk factors; use symptoms and anatomy to guide further cardiology evaluation |
This is a reasoning map, not a personalized treatment algorithm. Symptoms, prior events, pregnancy, age, comorbidities, and medication tolerance can change the decision.
Use imaging to answer a narrower question
Imaging is most valuable when the result can change what you do. Coronary artery calcium, or CAC, measures calcified coronary plaque and is a strong risk reclassifier. A score of zero can lower near-term risk in many adults, but it does not prove there is no non-calcified plaque, no familial hypercholesterolemia, no Lp(a)-related risk, or no lifetime exposure problem. Younger people have also had less time to calcify plaque.
Coronary CT angiography, or CCTA, shows coronary anatomy, stenosis, and both calcified and non-calcified plaque. It has a strong diagnostic role in chest-pain pathways and can be useful selectively in prevention when anatomy will change management. It is not a universal screening test. Contrast, radiation, incidental findings, scan quality, interpretation, and downstream testing are part of the decision.
Quantitative AI plaque analysis can add measurement detail to CCTA, but it is a measurement layer, not an oracle. Vendor variability, scan quality, human confirmation, thresholds for tiny plaque volumes, and the clinical value of serial scanning remain important limitations.
Protocol
What cardiovascular imaging can and cannot answer
CAC scan
- Best question
- Is there calcified coronary plaque, and does it reclassify risk?
- Important limitation
- Does not show non-calcified plaque or coronary stenosis; zero is not a lifetime-risk eraser
CCTA
- Best question
- What is the coronary anatomy, stenosis, total plaque burden, and plaque composition?
- Important limitation
- Not universal screening; requires contrast, radiation, expert interpretation, and a plan for incidental findings
Quantitative CCTA plaque analysis
- Best question
- Can plaque burden and composition be measured more consistently?
- Important limitation
- Software and scan variability remain; selective use with human oversight is essential
Carotid ultrasound
- Best question
- Is there carotid plaque outside the coronary circulation?
- Important limitation
- Carotid plaque is more useful than CIMT alone and is not interchangeable with coronary anatomy
Stress testing
- Best question
- Does exercise or medication provoke ischemia or a flow-limiting problem?
- Important limitation
- A normal test does not exclude non-obstructive plaque
| Test | Best question | Important limitation |
|---|---|---|
| CAC scan | Is there calcified coronary plaque, and does it reclassify risk? | Does not show non-calcified plaque or coronary stenosis; zero is not a lifetime-risk eraser |
| CCTA | What is the coronary anatomy, stenosis, total plaque burden, and plaque composition? | Not universal screening; requires contrast, radiation, expert interpretation, and a plan for incidental findings |
| Quantitative CCTA plaque analysis | Can plaque burden and composition be measured more consistently? | Software and scan variability remain; selective use with human oversight is essential |
| Carotid ultrasound | Is there carotid plaque outside the coronary circulation? | Carotid plaque is more useful than CIMT alone and is not interchangeable with coronary anatomy |
| Stress testing | Does exercise or medication provoke ischemia or a flow-limiting problem? | A normal test does not exclude non-obstructive plaque |
Do not use serial CAC as a simple treatment-response score. Successful plaque stabilization can increase calcium density even while risk falls.
Lower exposure before the 10-year risk score turns red
Atherosclerosis is an exposure-over-time disease. Cohort data show that cumulative LDL-C during young adulthood and middle age predicts later coronary disease independently of a single midlife measurement. Human genetics tells the same story from another angle: modest lifelong reductions in LDL can produce much larger risk reductions than an identical numerical change started after decades of exposure.
Randomized trials show that lowering LDL-C reduces events. Across the Cholesterol Treatment Trialists' meta-analysis, each 1 mmol/L, or about 39 mg/dL, LDL-C reduction produced roughly a one-fifth reduction in major vascular events over the trial periods studied. The absolute benefit is larger when baseline risk is higher, but the biology does not suddenly begin at the moment a calculator crosses a threshold.
Guidelines are useful anchors, not a substitute for lifetime-risk judgment. The 2026 ACC/AHA guideline brought back LDL-C and non-HDL-C goals, uses PREVENT-ASCVD for 10- and 30-year risk, recommends earlier treatment consideration with LDL-C at least 160 mg/dL or strong premature family history in young adults, and uses CAC selectively when a treatment decision remains uncertain.
Protocol
2026 LDL-C goal anchors
Low, borderline, or intermediate primary-prevention risk
- LDL-C goal anchor
- Generally <100 mg/dL
- How I interpret it
- Risk enhancers, lifetime exposure, Lp(a), family history, diabetes, CKD, or plaque can justify greater intensity
High primary-prevention risk, generally PREVENT-ASCVD ≥10%
- LDL-C goal anchor
- <70 mg/dL
- How I interpret it
- Treat the absolute risk and the needed percentage reduction, not the number in isolation
LDL-C ≥190 mg/dL or likely familial hypercholesterolemia
- LDL-C goal anchor
- At least <100 mg/dL and usually ≥50% reduction
- How I interpret it
- Earlier and often combination therapy is reasonable; additional risk frequently supports a lower goal
Clinical ASCVD, not very high risk
- LDL-C goal anchor
- <70 mg/dL
- How I interpret it
- Most people with prior events will meet criteria for the more intensive category
Clinical ASCVD at very high recurrent-event risk
- LDL-C goal anchor
- <55 mg/dL
- How I interpret it
- Use outcome-proven combination therapy as needed to reach the goal safely and durably
| Clinical context | LDL-C goal anchor | How I interpret it |
|---|---|---|
| Low, borderline, or intermediate primary-prevention risk | Generally <100 mg/dL | Risk enhancers, lifetime exposure, Lp(a), family history, diabetes, CKD, or plaque can justify greater intensity |
| High primary-prevention risk, generally PREVENT-ASCVD ≥10% | <70 mg/dL | Treat the absolute risk and the needed percentage reduction, not the number in isolation |
| LDL-C ≥190 mg/dL or likely familial hypercholesterolemia | At least <100 mg/dL and usually ≥50% reduction | Earlier and often combination therapy is reasonable; additional risk frequently supports a lower goal |
| Clinical ASCVD, not very high risk | <70 mg/dL | Most people with prior events will meet criteria for the more intensive category |
| Clinical ASCVD at very high recurrent-event risk | <55 mg/dL | Use outcome-proven combination therapy as needed to reach the goal safely and durably |
These are population-level guideline anchors. ApoB thresholds can refine residual particle risk, and an individual's target must account for diagnosis, age, prior events, comorbidities, pregnancy, tolerance, and shared decision-making.
Lifestyle changes the terrain and can lower ApoB, but it has a ceiling
Lifestyle is foundational because it can change several causal pathways at once: ApoB, remnants, blood pressure, insulin resistance, visceral adiposity, endothelial function, smoking exposure, sleep apnea, fitness, and inflammation. The most reliable lipid lever is replacing saturated fat with unsaturated fat, not simply eating less fat. Soluble fiber, minimally processed plant foods, nuts, legumes, fish, and a Mediterranean or Portfolio-style pattern can add benefit.
Exercise often improves triglycerides, insulin sensitivity, blood pressure, fitness, and body composition more than it changes LDL-C. That does not make exercise secondary. It means exercise and lipid-lowering medication can be solving different parts of the disease model.
The ceiling matters. Lifestyle may be enough for a modest elevation in a lower-risk person. It is often not enough for LDL-C around 190 mg/dL, familial hypercholesterolemia, high Lp(a), established plaque, prior events, or a large ApoB reduction requirement. Needing medication is not a moral failure, and taking medication does not make lifestyle optional.
Protocol
The prevention stack: what each lever is best at
Replace saturated fat with unsaturated fat
- Primary job
- Lower LDL-C and ApoB in responders while improving overall diet quality
- What not to overclaim
- Diet response varies, and severe genetic elevation usually needs more
Increase soluble fiber and plant-food quality
- Primary job
- Modest LDL-C reduction, better satiety, glycemic control, and bowel health
- What not to overclaim
- A supplement cannot rescue a diet pattern or replace necessary therapy
Reduce visceral adiposity when present
- Primary job
- Improve triglycerides, insulin resistance, blood pressure, liver risk, and often ApoB
- What not to overclaim
- Scale weight alone does not show fat distribution or preserve muscle
Aerobic and resistance exercise
- Primary job
- Improve fitness, insulin sensitivity, blood pressure, triglycerides, body composition, and reserve
- What not to overclaim
- Exercise usually moves LDL-C less than it moves overall cardiovascular risk
Stop smoking and avoid combustible exposure
- Primary job
- Reduce endothelial injury, thrombosis, inflammation, and event risk
- What not to overclaim
- A favorable lipid panel does not cancel tobacco risk
Treat blood pressure, diabetes, CKD, and sleep apnea
- Primary job
- Reduce artery-wall force and major non-lipid accelerants
- What not to overclaim
- Lowering ApoB does not replace management of the rest of the terrain
| Lever | Primary job | What not to overclaim |
|---|---|---|
| Replace saturated fat with unsaturated fat | Lower LDL-C and ApoB in responders while improving overall diet quality | Diet response varies, and severe genetic elevation usually needs more |
| Increase soluble fiber and plant-food quality | Modest LDL-C reduction, better satiety, glycemic control, and bowel health | A supplement cannot rescue a diet pattern or replace necessary therapy |
| Reduce visceral adiposity when present | Improve triglycerides, insulin resistance, blood pressure, liver risk, and often ApoB | Scale weight alone does not show fat distribution or preserve muscle |
| Aerobic and resistance exercise | Improve fitness, insulin sensitivity, blood pressure, triglycerides, body composition, and reserve | Exercise usually moves LDL-C less than it moves overall cardiovascular risk |
| Stop smoking and avoid combustible exposure | Reduce endothelial injury, thrombosis, inflammation, and event risk | A favorable lipid panel does not cancel tobacco risk |
| Treat blood pressure, diabetes, CKD, and sleep apnea | Reduce artery-wall force and major non-lipid accelerants | Lowering ApoB does not replace management of the rest of the terrain |
For triglycerides at or above 1,000 mg/dL, the immediate clinical priority includes pancreatitis prevention and evaluation of secondary or genetic causes.
Choose medication by the job it needs to do
The medication question is not statin versus everything else. It is how much additional ApoB and LDL-C lowering is needed, which therapies have outcome evidence in a similar population, which risks matter for this person, and which regimen they can sustain.
Statins remain the foundation because they are inexpensive, potent, and supported by the broadest cardiovascular-outcomes evidence. Ezetimibe adds a complementary intestinal mechanism with low daily burden. Bempedoic acid provides oral outcome-proven therapy for statin-intolerant patients. PCSK9 antibodies produce large reductions with direct cardiovascular-outcomes evidence. Inclisiran solves a supervised-adherence problem with twice-yearly clinician administration, while its dedicated outcomes evidence is still maturing.
Lipfendra, or enlicitide, is the first oral PCSK9 inhibitor. It produced roughly 56 to 59 percent placebo-adjusted LDL-C reductions and about 50 percent ApoB reductions in Phase 3 trials. It is a potent new option, not automatic proof that statins or injections are obsolete. It must be taken in the morning on an empty stomach followed by a 30-minute wait before most food or drinks, and its product-specific cardiovascular-outcomes trial is ongoing.
Interactive treatment map
One LDL-receptor system, several intervention points
The therapies differ because they act at different points: absorption, synthesis, PCSK9 production, receptor recycling, or extracellular PCSK9 binding.
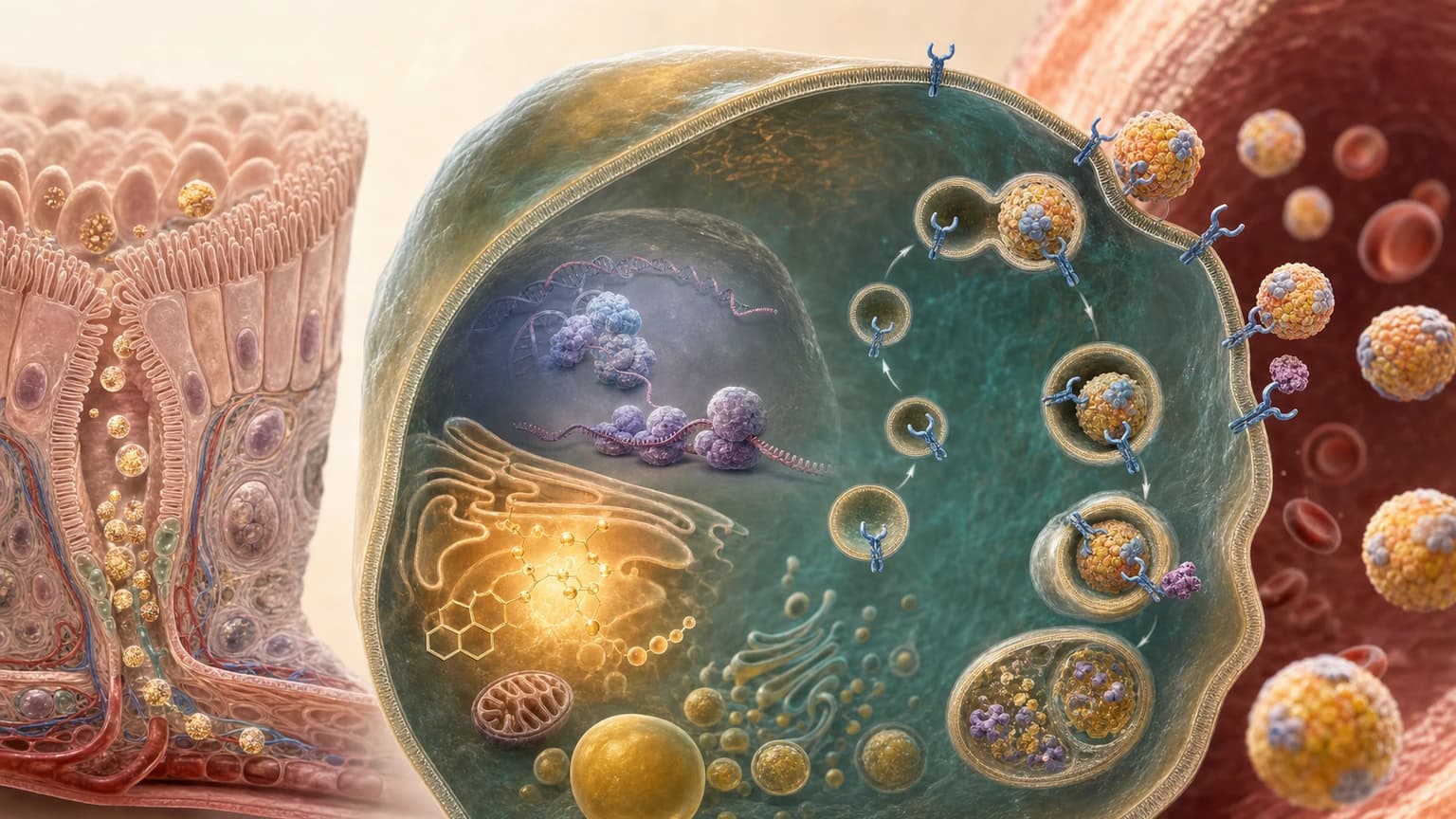
Mechanism is not outcomes evidence. Potency, administration burden, reversibility, access, and clinical evidence still differ by therapy.
Medication map
Medication mechanism map and evidence status
How to read this section
Compare the therapy, approximate scale of LDL-C lowering, and the evidence or practical tradeoff. These percentages are orientation, not a head-to-head outcomes ranking.
Statin
Typical LDL-C effect
About 30% to ≥50%, depending on intensity
Outcome evidence and main tradeoff
Extensive event-reduction evidence; muscle symptoms, interactions, and a small diabetes-risk signal require context
Ezetimibe
Typical LDL-C effect
About 15% to 25%
Outcome evidence and main tradeoff
Direct add-on event evidence after acute coronary syndrome; modest potency but low cost and generally low burden
Bempedoic acid
Typical LDL-C effect
About 20%
Outcome evidence and main tradeoff
Direct event evidence in statin-intolerant high-risk adults; consider uric acid, gout, gallstones, and tendon warnings
PCSK9 antibody: evolocumab or alirocumab
Typical LDL-C effect
About 50% to 60%
Outcome evidence and main tradeoff
Direct event evidence in established disease and high-risk first-event prevention; self-injection and coverage are practical barriers
Inclisiran
Typical LDL-C effect
About 50%
Outcome evidence and main tradeoff
Twice-yearly clinician dosing after initiation; product-specific outcomes trials are ongoing
Lipfendra / enlicitide
Typical LDL-C effect
About 56% to 59% vs placebo
Outcome evidence and main tradeoff
First oral PCSK9 inhibitor; daily fasting choreography and product-specific outcomes still pending
Typical effects are approximate and depend on baseline therapy, adherence, genetics, and trial population. Do not compare percentages as if they came from one head-to-head outcomes trial.
Statin symptoms are a troubleshooting problem, not a dead end
Muscle symptoms deserve a real evaluation. The right response is not to dismiss the patient, and it is not to conclude that every statin at every dose is impossible after one trial. Symptoms can be related to the statin, an interaction, dose, thyroid disease, a training change, another medication, or an unrelated musculoskeletal problem. Severe pain, weakness, dark urine, fever, or systemic illness requires prompt assessment.
A structured approach can include reviewing interacting drugs and grapefruit exposure, checking the timing of symptoms, measuring CK when clinically indicated, pausing and rechallenging, trying a different statin, using a lower or intermittent dose, and combining a smaller tolerated dose with ezetimibe or another nonstatin. Pharmacogenomics can be useful in selected cases, especially with a history suggesting transporter-related myopathy, but it is not a universal prerequisite.
The goal is not loyalty to a molecule. The goal is durable reduction of causal particle exposure by a route the patient can tolerate.
Do not ignore severe symptomsMarked weakness, dark urine, severe pain, fever, or systemic illness warrants urgent clinical assessment.
Do not abandon the targetIf one statin regimen fails, alternate statins, doses, combinations, and nonstatins remain available.
Do not let nocebo become dismissalBlinded trials show some symptom burden is expectation-related, but the patient's experience still needs a respectful plan.
Monitor the response, not just the prescription
After a meaningful medication or dietary change, I generally want the same lipid markers repeated after enough time to see the effect, often around 6 to 12 weeks. Once the regimen is stable and goals are met, every 6 to 12 months is common. Earlier testing may be appropriate with severe dyslipidemia, pregnancy planning, side effects, adherence questions, rapid titration, or a high-risk clinical situation.
Monitoring should answer four questions: Did the marker move by the expected amount? Is the patient actually taking the regimen as intended? Is it tolerated? Does the residual risk justify another step? For Lipfendra, administration timing is part of adherence. For injections, storage, technique, coverage interruptions, and missed doses matter. For any therapy, a smaller-than-expected response should trigger a check of adherence, secondary causes, biology, and the diagnosis before simply stacking another drug.
Routine CK or liver-enzyme testing is not necessary forever in every asymptomatic statin user. Baseline clinical context and symptom-triggered testing matter. Serial CAC is also not a treatment-response biomarker. If imaging is repeated, there should be a specific question and a realistic interval, not scan-chasing.
Protocol
A practical monitoring protocol
Before treatment
- What to check
- Lipid panel, non-HDL-C, ApoB when useful, Lp(a) once, blood pressure, glucose/A1c, kidney and liver context, medications, pregnancy plans, and symptoms
- Decision
- Confirm the phenotype, risk, needed reduction, safety constraints, and preferred route
About 6 to 12 weeks after a change
- What to check
- Repeat the same lipid targets; review adherence, administration, symptoms, and expected percentage change
- Decision
- Continue, troubleshoot, titrate, or add therapy
Stable regimen
- What to check
- Usually repeat labs every 6 to 12 months with ongoing blood pressure and metabolic-risk review
- Decision
- Protect durability and detect drift or new risk
New symptoms or poor response
- What to check
- Targeted CK, liver, thyroid, medication-interaction, adherence, or secondary-cause evaluation as indicated
- Decision
- Do not reflexively blame or ignore the drug; identify the mechanism of failure
| Moment | What to check | Decision |
|---|---|---|
| Before treatment | Lipid panel, non-HDL-C, ApoB when useful, Lp(a) once, blood pressure, glucose/A1c, kidney and liver context, medications, pregnancy plans, and symptoms | Confirm the phenotype, risk, needed reduction, safety constraints, and preferred route |
| About 6 to 12 weeks after a change | Repeat the same lipid targets; review adherence, administration, symptoms, and expected percentage change | Continue, troubleshoot, titrate, or add therapy |
| Stable regimen | Usually repeat labs every 6 to 12 months with ongoing blood pressure and metabolic-risk review | Protect durability and detect drift or new risk |
| New symptoms or poor response | Targeted CK, liver, thyroid, medication-interaction, adherence, or secondary-cause evaluation as indicated | Do not reflexively blame or ignore the drug; identify the mechanism of failure |
Monitoring frequency is individualized. This table is educational and does not replace a clinician who knows the diagnosis and medication history.
Know when to involve a lipid specialist or preventive cardiologist
Many lipid decisions can be managed in primary care. Specialist input becomes especially valuable when the diagnosis, target, medication architecture, or imaging question is not straightforward. The point of referral is not to outsource prevention. It is to solve a problem that needs deeper phenotyping, combination therapy, or disease-specific judgment.
Severe elevationLDL-C at or above 190 mg/dL, suspected familial hypercholesterolemia, or very high ApoB despite treatment.
Premature diseaseMyocardial infarction, stroke, revascularization, or meaningful plaque at a young age.
Inherited riskVery high Lp(a), strong premature family history, possible genetic dyslipidemia, or aortic-valve disease context.
Treatment complexityRepeated medication intolerance, poor response, multi-drug combinations, pregnancy planning, or access barriers.
Triglyceride emergencySevere or recurrent hypertriglyceridemia, pancreatitis, or suspected familial chylomicronemia.
Imaging conflictSymptoms, CAC, CCTA, stress testing, and laboratory risk do not tell a coherent story.
What I would do first
For an adult who wants a serious prevention baseline, I would begin with blood pressure, a standard lipid panel, non-HDL-C, ApoB, Lp(a) once, A1c or fasting glucose, kidney function, smoking status, medication review, and a three-generation family history focused on premature heart attack, stroke, revascularization, sudden death, and known extreme cholesterol.
If the numbers are favorable and the family history is quiet, I would focus on durable lifestyle, blood pressure, metabolic health, fitness, and periodic reassessment. If ApoB or LDL-C is high, Lp(a) is elevated, family history is strong, LDL-C is near or above 190 mg/dL, or plaque is already present, I would not wait for symptoms. I would estimate the reduction actually needed, start the lowest-burden plan likely to reach it, and verify the response.
If the treatment decision remains genuinely uncertain, CAC can be a useful tie-breaker in the appropriate age group. If symptoms or a specific anatomical question exist, CCTA or another cardiology pathway may be more relevant. I would not order every test simply because it exists.
My honest take
I use a PCSK9 inhibitor in my own care. My untreated LDL-C was 192 mg/dL, my family history is severe, and statins gave me muscle symptoms. Repatha lowered my LDL-C to roughly 40 mg/dL. I do not do this because I think every adult needs the same number or the same drug. I do it because my lifetime exposure and family endpoint make the tradeoff reasonable to me.
I am excited about Lipfendra because a potent pill may remove injection friction for many people. I would not automatically switch a working, outcome-proven regimen just because the new route sounds easier. The pill has fasting choreography, product-specific outcomes are pending, and access will matter. The best treatment is the one that lowers ApoB enough, has evidence proportional to the person's risk, fits daily life, and remains tolerable and sustainable.
The central prevention mistake is waiting for atherosclerosis to become symptomatic before treating its causes. The second mistake is reducing the whole disease to one lab value. Measure the layer you are trying to change, act early enough for time to work in your favor, and close the loop with repeat data.
Clinical lens
How I’d decide
Use this section as a second pass after the main answer, not as homework before you know what the page is saying.
Who it’s for
Adults who want a serious cardiovascular-prevention baseline; people with high LDL-C, ApoB, triglycerides, or Lp(a); strong family history; diabetes or CKD; suspected familial hypercholesterolemia; statin symptoms; positive CAC or CCTA; or uncertainty about how to combine lifestyle, medication, and imaging.
Who should skip it
This is not a self-treatment protocol for chest pain, neurologic symptoms, pregnancy, severe medication reactions, triglycerides near or above 1,000 mg/dL, or known cardiovascular disease without clinician oversight. Acute chest pressure, shortness of breath, fainting, or stroke symptoms require urgent evaluation rather than more prevention testing.
Measure before / after
Start with blood pressure, standard lipid panel, non-HDL-C, ApoB, Lp(a) at least once, glucose or A1c, kidney function, smoking status, medication review, and family history. Repeat the same lipid targets about 6 to 12 weeks after a meaningful treatment change, then generally every 6 to 12 months once stable. Use CAC, CCTA, carotid imaging, or stress testing only for a defined question.
What I’d do first
I would identify the particle burden and inherited risk first, estimate how much lowering is actually needed, start the lowest-burden durable plan likely to reach it, and verify the response. I would not wait for symptoms when LDL-C is near 190 mg/dL, family history is severe, Lp(a) is high, or plaque is already present. I would also not order every advanced test simply because it exists.
What would change my mind
New cardiovascular-outcomes data, a large discrepancy between expected and observed treatment response, new plaque or symptoms, pregnancy plans, a major adverse effect, a change in kidney or metabolic disease, or evidence that a supposedly convenient regimen is not being followed would all change the plan.
Frequently Asked Questions
Can atherosclerosis be reversed?
Sometimes plaque burden can regress modestly, especially non-calcified or lipid-rich plaque, but 'reversal' is an imprecise promise. Intensive ApoB and LDL-C lowering can slow progression, reduce some plaque volume, and shift plaque toward a more stable, densely calcified phenotype. Event reduction matters more than making a scan look clean. CAC can rise as plaque becomes denser, so serial CAC should not be used as a simple scorecard for treatment success.
Is ApoB more important than LDL cholesterol?
ApoB often gives the better estimate of atherogenic particle burden because every LDL, remnant, IDL, and Lp(a) particle carries one ApoB molecule. LDL-C measures cholesterol mass inside LDL particles. When the two are discordant, risk often tracks more closely with ApoB, especially with high triglycerides, diabetes, insulin resistance, obesity, or lipid treatment. LDL-C remains useful and guideline-anchored; ApoB adds precision rather than making the standard lipid panel obsolete.
What should my ApoB level be?
There is no single target for everyone. The 2024 National Lipid Association consensus lists ApoB treatment-intensification thresholds around 90 mg/dL for borderline or intermediate risk, 70 mg/dL for high risk, and 60 mg/dL for very high risk. These are clinical anchors, not a diagnosis by themselves. Established ASCVD, plaque, Lp(a), diabetes, CKD, familial hypercholesterolemia, age, and treatment tolerance can justify a lower or different target.
Should everyone get lipoprotein(a) tested?
The 2026 ACC/AHA guideline recommends measuring Lp(a) at least once in adulthood. It is mostly genetically determined and usually stable enough that frequent repeat testing is unnecessary unless a specific treatment or clinical question changes. A level at or above 125 nmol/L, or 50 mg/dL, is considered a risk enhancer; very high levels carry greater risk. The immediate action is usually stronger control of ApoB, blood pressure, smoking, diabetes, kidney disease, and other modifiable risks.
Does a coronary calcium score of zero mean I do not need cholesterol treatment?
No. CAC zero can lower near-term risk in many adults, but it does not show non-calcified plaque and does not erase lifetime exposure, familial hypercholesterolemia, high Lp(a), diabetes, smoking, or a strong family history. It is also less reassuring at younger ages because plaque has had less time to calcify. Use CAC zero as one piece of risk reclassification, not a universal permission slip to ignore high ApoB or LDL-C.
When is CCTA more useful than a calcium scan?
CCTA is more useful when the question is coronary anatomy, stenosis, symptoms, or the presence and composition of both calcified and non-calcified plaque. CAC is a simpler non-contrast test for calcified plaque burden and risk reclassification. CCTA is not a universal screening test because it involves contrast, radiation, scan-quality requirements, incidental findings, and downstream decisions. The right test is the one whose answer will change management.
Can diet and exercise lower ApoB enough without medication?
Sometimes. Replacing saturated fat with unsaturated fat, increasing soluble fiber and plant-food quality, losing visceral fat when present, and improving metabolic health can lower ApoB and LDL-C. The size of the response varies. Lifestyle alone is often insufficient for LDL-C around 190 mg/dL, familial hypercholesterolemia, established plaque, prior cardiovascular events, high Lp(a) with stacked risk, or a large required reduction. Medication and lifestyle solve complementary parts of the problem.
Do statins make coronary calcium worse?
Statins can increase plaque calcium density while reducing lipid-rich plaque, inflammation, progression, and cardiovascular events. That pattern is generally interpreted as stabilization, not treatment failure. It is one reason serial CAC is a poor treatment-response test. The clinically important outcomes are lower ApoB and LDL-C, lower event risk, controlled blood pressure and metabolic disease, and symptom-guided evaluation when needed.
What if I get muscle symptoms from a statin?
Muscle symptoms should be evaluated rather than dismissed or treated as proof that all lipid therapy is impossible. Review timing, dose, interacting drugs, thyroid disease, exercise changes, and other causes. A clinician may pause and rechallenge, try a different statin, use a lower or intermittent dose, or combine a smaller tolerated dose with ezetimibe, bempedoic acid, or a PCSK9-directed therapy. Severe weakness, dark urine, fever, or systemic illness needs prompt assessment.
Should I take Lipfendra instead of a statin?
Usually not simply because it is newer or oral. In CORALreef Lipids, 97 percent of participants were taking a statin, so the pivotal trial mainly tested enlicitide as add-on therapy. Statins remain inexpensive and have decades of cardiovascular-outcomes evidence. Lipfendra may be useful when someone cannot tolerate an adequate statin regimen, remains above target despite other therapy, or needs PCSK9-level potency without an injection, but its product-specific outcomes trial is still underway.
Should I take Lipfendra on top of Repatha or another injectable PCSK9 drug?
Not as a routine stack. Enlicitide and the antibodies Repatha and Praluent all block the circulating PCSK9-LDL-receptor interaction, and the pivotal Lipfendra trial excluded people taking other PCSK9 inhibitors. We therefore do not have established evidence that combining them adds meaningful LDL lowering, improves outcomes, or is the best use of two drugs aimed at the same step. Inclisiran reduces PCSK9 production upstream, but combining it with enlicitide is also not an established routine strategy. In most cases the choice is one PCSK9 route, with a complementary mechanism considered if more lowering is still needed.
References & citations
- 1.2026 ACC/AHA multisociety guideline on the management of dyslipidemia: Top Things to Know
- 2.National Lipid Association Expert Clinical Consensus: Role of ApoB in cardiovascular risk management, 2024
- 3.Sehayek et al. ApoB, LDL-C, and non-HDL-C as markers of cardiovascular risk, Journal of Clinical Lipidology, 2025
- 4.Zhang et al. Cumulative LDL-C exposure in young adulthood and middle age and incident cardiovascular disease, JAMA Cardiology, 2021
- 5.Cholesterol Treatment Trialists' Collaboration. More intensive LDL lowering in 170,000 participants, The Lancet, 2010
- 6.Mehta et al. Independent association of Lp(a) and coronary artery calcium with ASCVD risk, JACC, 2022
- 7.SCOT-HEART Investigators. Coronary CT angiography and 5-year risk of myocardial infarction, NEJM, 2018
- 8.ACC Scientific Statement: Quantitative coronary plaque analysis in clinical practice, 2025
- 9.FOURIER: Evolocumab and clinical outcomes in patients with cardiovascular disease, NEJM, 2017
- 10.VESALIUS-CV: Evolocumab in patients without a previous myocardial infarction or stroke, NEJM, 2026
- 11.IMPROVE-IT: Ezetimibe added to statin therapy after acute coronary syndromes, NEJM, 2015
- 12.CLEAR Outcomes: Bempedoic acid and cardiovascular outcomes in statin-intolerant patients, NEJM, 2023
- 13.CORALreef Lipids: A placebo-controlled trial of the oral PCSK9 inhibitor enlicitide, NEJM, 2026
- 14.FDA-approved Lipfendra prescribing information
- 15.CORALreef Outcomes cardiovascular-outcomes trial registry
Related Guides
Next step
Turn the guide into the right next decision.
If this page raised a real clinical question, start with the practice details. If you are still learning, get the weekly letter. If you are comparing tests, use the testing hub before buying another panel.