The Longevity Audit: What to Check Before You Optimize
A longevity audit is prevention triage: close symptoms and abnormal results first, then blood pressure, atherogenic lipids, metabolic risk, screening, sleep apnea when suspected, kidney/liver risk, and asymmetric safety loops—including tobacco/nicotine exposure—before advanced optimization.
Order matters
Start with warning lights and fatal loops. Put tobacco/nicotine, alcohol, medication, vaccine, and safety issues in the asymmetric-risk review. Add advanced tests only when they change care.
Use ranges wisely
Some cutoffs diagnose disease; others are risk anchors. The useful question is what result changes the next decision.
Build reserve
After preventable risk is handled, fitness, strength, sleep, nutrition, sensory health, and social connection become the healthspan work.
Short answer
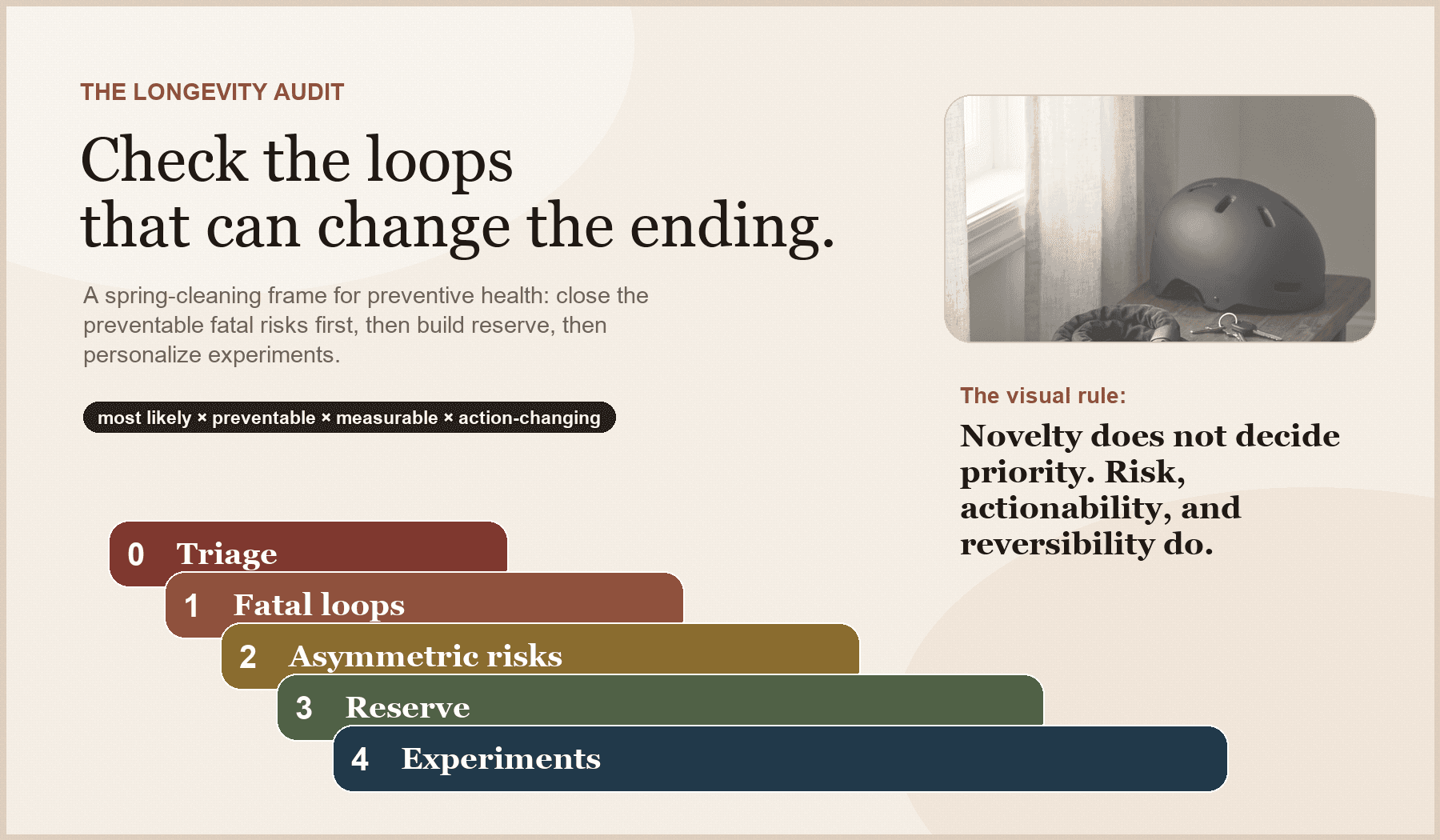
A longevity audit is health spring cleaning with triage. It is not a scavenger hunt for the newest biomarker. It asks: what is the most preventable, measurable thing most likely to shorten my life or shrink my independence, and have I actually closed that loop?
The order matters. First, follow up symptoms and known abnormal results. Then close the fatal loops: blood pressure, atherogenic lipoproteins, metabolic risk, age- and risk-appropriate cancer screening, sleep apnea when suspected, and kidney/liver/vascular risk. Put tobacco and nicotine exposure in the asymmetric-risk review: the downside is huge, the first move is concrete, and it deserves more than a throwaway checkbox.
Advanced biomarkers, hormones, wearables, genetics, MCED blood tests, whole-body MRI, rapamycin debates, and n=1 experiments move up only when they would change a decision and the follow-up plan is real. Interesting is not the same as first.
Protocol
Longevity audit priority order
Priority tier
What belongs here
Why it comes first
Examples
Priority tier
1. Warning lights
What belongs here
Symptoms, known abnormal tests, clinician-requested follow-up
Why it comes first
Already abnormal beats speculative optimization
Examples
Chest pain, blood in stool, positive FIT, abnormal mammogram, rising creatinine, unexplained anemia
Priority tier
2. Fatal loops
What belongs here
Silent, common, preventable drivers of early morbidity and mortality
Why it comes first
High absolute risk + high actionability
Examples
Blood pressure, ApoB/LDL/Lp(a), metabolic risk, cancer screening, sleep apnea, kidney/liver risk
Priority tier
3. Asymmetric safeguards
What belongs here
Low-friction steps that prevent large downside
Why it comes first
Cheap, boring, often skipped
Examples
Tobacco/nicotine exposure, alcohol floor, seat belts, helmets, fall prevention, medication review, vaccines, aspirin review
Priority tier
4. Physiologic reserve
What belongs here
Capacity to tolerate illness, aging, travel, stress, and recovery
Why it comes first
Healthspan depends on reserve, not just absence of disease
Examples
Aerobic fitness, strength, balance, sleep, protein/fiber, hearing/vision, social connection
Priority tier
5. Advanced / personalized tools
What belongs here
Tests or interventions with context-dependent value
Why it comes first
Useful when they change a decision after the basics and follow-up plan are real
Examples
MCED, whole-body MRI, CGM, CAC, hormones, genomics, biological-age clocks, microbiome reports, supplements
How to use this guide without turning it into homework
Use the tables as anchors, not as a diagnosis engine. Some ranges are formal diagnostic cut points; others are practical decision thresholds or risk-enhancing signals. Targets can change with age, pregnancy history, kidney disease, diabetes, ASCVD risk, medications, symptoms, and personal tradeoffs.
The useful question is not “is this number perfect?” It is “does this result change what I do next?” If the answer is no, it may not deserve top billing.
Educational, not personal medical advice. If you have symptoms, a known abnormal result, or a clinician has asked you to repeat or follow up something, that outranks this guide.
Why most longevity checklists get the order wrong
A lot of longevity advice is organized by novelty. That is how people end up comparing epigenetic clocks while they do not know their home blood pressure, debating supplement stacks while colorectal screening is overdue, or wearing three devices while weekend alcohol is wrecking sleep, mood, reflux, and blood pressure.
The problem is not curiosity. The problem is sequence.
A useful audit uses this formula: priority = absolute risk × preventability × actionability × evidence quality × personalization.
That formula pushes boring, measurable, evidence-backed risks above shiny objects. It also keeps the audit personal. A 35-year-old cyclist with a strong family history of early heart disease should not have the same first five priorities as a 68-year-old with falls, insomnia, hypertension, and ten medications.
Where the hallmarks of aging fit

Hallmarks explain the biology. The audit filter decides what belongs in care.
The hallmarks of aging are the mechanism map underneath the audit: genomic instability, telomere attrition, epigenetic alterations, loss of proteostasis, disabled macroautophagy, deregulated nutrient-sensing, mitochondrial dysfunction, cellular senescence, stem-cell exhaustion, altered intercellular communication, chronic inflammation, and dysbiosis.
That biology matters because it explains why the “boring” levers are not boring. DNA damage, telomeres, and senescence point toward cancer risk, tobacco and UV exposure, infection prevention, and abnormal-test follow-through. Nutrient sensing, mitochondria, autophagy, and proteostasis point toward insulin resistance, visceral fat, fitness, muscle, sleep, protein, alcohol, and medication context. Inflammation, dysbiosis, altered signaling, and stem-cell exhaustion point toward sleep apnea, oral and infection risk, chronic inflammatory disease, fiber, frailty, bone, recovery, and immune vulnerability.
Mechanisms are useful when they translate into a human proxy, a decision-changing metric, and a lower-harm action. Otherwise they belong in the research file, not at the top of your weekend checklist.
First: symptoms are not audit items
This guide is for prevention and risk review in people who are generally stable. It is not a substitute for medical care.
If you have chest pain, shortness of breath out of proportion, fainting, new neurologic symptoms, a new severe headache, unexplained weight loss, blood in stool, persistent fevers, abnormal bleeding, new focal weakness, severe depression, suicidal thoughts, or another concerning symptom, do not turn it into a longevity project. Get evaluated.
Same for the things already trying to get your attention: a positive stool test, abnormal mammogram, persistently high blood pressure, rising creatinine, unexplained anemia, abnormal bleeding, or a lab your clinician asked you to repeat.
The first audit question is simple: is there already a warning light I am trying to rebrand as optimization? If yes, start there.
Tier 1: close the fatal loops
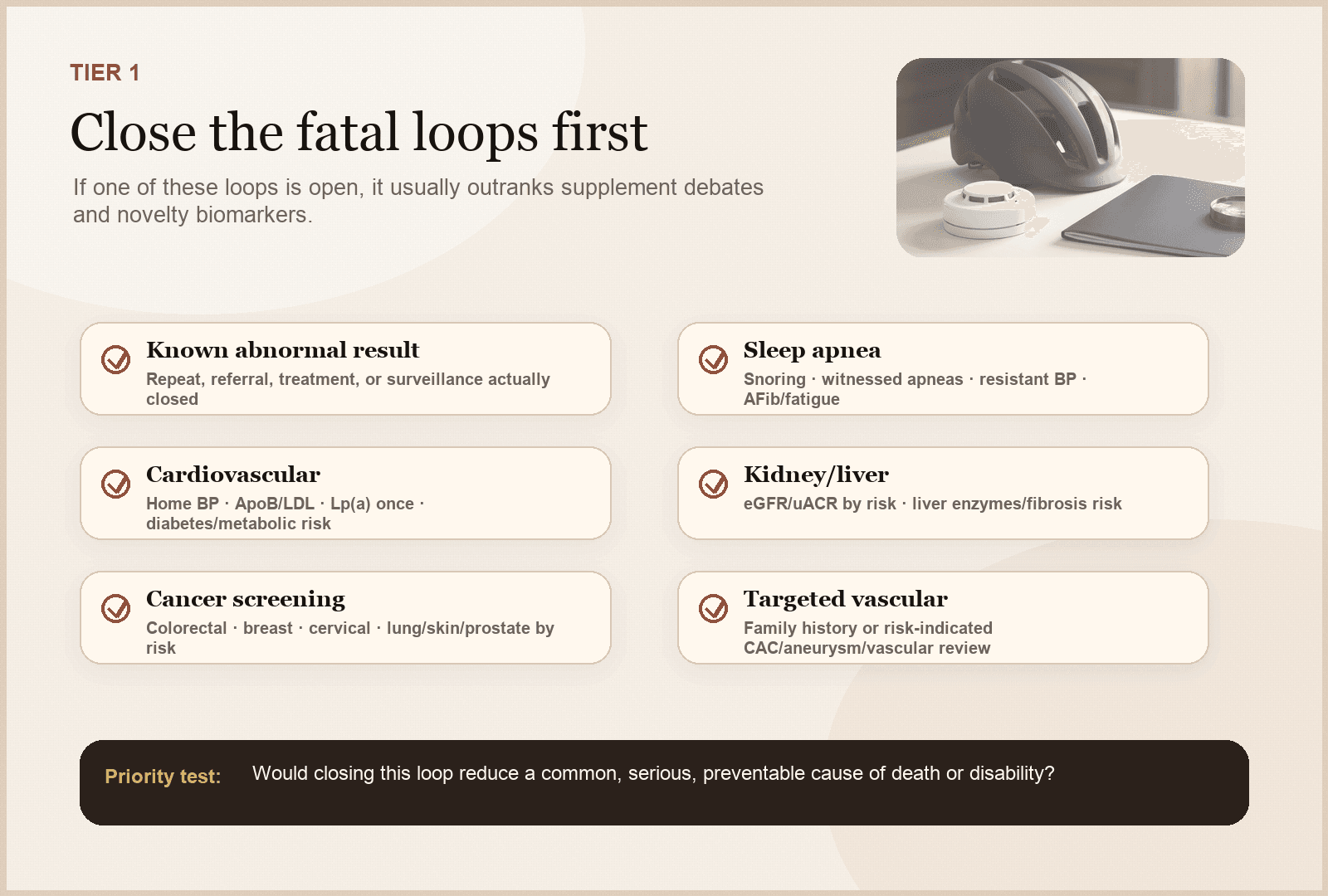
If a fatal-risk loop is open, close that branch before adding optimization projects.
These are the risks and conditions that often kill early, silently, or preventably. They usually deserve attention before exotic optimization.
1. Blood pressure: the highest-ROI home metric
Blood pressure is common, silent, measurable, actionable, and easy to measure badly. It drives stroke, heart disease, heart failure, kidney disease, vascular brain injury, and pregnancy-related risk patterns.
The audit question is not “what was one clinic reading?” It is: do I know my usual home blood pressure, measured with the right cuff and technique, and do I have a plan if it is repeatedly high?
Protocol
Blood pressure ranges to know
Normal
- Typical anchor
- <120 systolic and <80 diastolic
- What it means for the audit
- Good baseline if measured correctly; still repeat over time
- Next move
- Keep a validated cuff, repeat periodically, protect sleep/activity/nutrition
Elevated
- Typical anchor
- 120–129 systolic and <80 diastolic
- What it means for the audit
- Early warning zone; do not wait until it is “real hypertension” to care
- Next move
- Standardize home readings, reduce sodium/alcohol if relevant, increase activity, recheck
Stage 1 hypertension
- Typical anchor
- 130–139 systolic or 80–89 diastolic
- What it means for the audit
- Risk context decides intensity; confirmation matters
- Next move
- Confirm with home/ambulatory readings and discuss ASCVD risk, lifestyle, and medication threshold
Stage 2 hypertension
- Typical anchor
- ≥140 systolic or ≥90 diastolic
- What it means for the audit
- High-priority fatal loop
- Next move
- Confirm promptly and create an actual treatment plan
Severe range
- Typical anchor
- >180 systolic and/or >120 diastolic
- What it means for the audit
- Not a longevity spreadsheet item
- Next move
- Repeat after 1 minute; if symptoms such as chest pain, shortness of breath, neurologic symptoms, vision change, weakness, or trouble speaking: call emergency services
| Range | Typical anchor | What it means for the audit | Next move |
|---|---|---|---|
| Normal | <120 systolic and <80 diastolic | Good baseline if measured correctly; still repeat over time | Keep a validated cuff, repeat periodically, protect sleep/activity/nutrition |
| Elevated | 120–129 systolic and <80 diastolic | Early warning zone; do not wait until it is “real hypertension” to care | Standardize home readings, reduce sodium/alcohol if relevant, increase activity, recheck |
| Stage 1 hypertension | 130–139 systolic or 80–89 diastolic | Risk context decides intensity; confirmation matters | Confirm with home/ambulatory readings and discuss ASCVD risk, lifestyle, and medication threshold |
| Stage 2 hypertension | ≥140 systolic or ≥90 diastolic | High-priority fatal loop | Confirm promptly and create an actual treatment plan |
| Severe range | >180 systolic and/or >120 diastolic | Not a longevity spreadsheet item | Repeat after 1 minute; if symptoms such as chest pain, shortness of breath, neurologic symptoms, vision change, weakness, or trouble speaking: call emergency services |
If you buy only one home device, make it a validated upper-arm blood pressure cuff. Not sexy. Extremely useful. The cuff does not care about your supplement drawer.
2. Atherogenic lipoproteins: LDL-C, non-HDL-C, ApoB, and Lp(a)
The most common fatal surprise is often not a surprise biologically. It is years of blood pressure, ApoB-containing particles, glucose, inflammation, and family history adding up in the background.
Core questions: What are my LDL-C and non-HDL-C? Do I know ApoB if metabolic risk, high triglycerides, insulin resistance, or discordance is possible? Have I checked Lp(a) once in adulthood? Is there premature ASCVD, stroke, sudden death, or very high cholesterol in my family? Would CAC change a treatment decision, or am I ordering it to feel thorough?
Protocol
Cardiovascular lab anchors
LDL-C
- Useful anchor
- LDL-C ≥190 mg/dL is a major red flag; lower targets depend on total risk
- Why it matters
- LDL is a causal atherogenic exposure over time
- What changes the plan
- Very high LDL, premature family history, diabetes, CKD, high 10-year risk, or existing ASCVD shifts intensity
Non-HDL-C
- Useful anchor
- Useful when triglycerides are elevated or LDL alone may understate particle burden
- Why it matters
- Captures cholesterol carried by ApoB-containing particles
- What changes the plan
- Discordance with LDL-C can support checking ApoB and treating the risk stack, not the prettiest number
ApoB
- Useful anchor
- ApoB ≥130 mg/dL is often treated as a risk-enhancing signal; lower targets are risk-dependent
- Why it matters
- Counts atherogenic particles more directly than LDL-C
- What changes the plan
- Especially useful with insulin resistance, high triglycerides, obesity, diabetes risk, or LDL/ApoB discordance
Lp(a)
- Useful anchor
- Check once in adulthood; ≥50 mg/dL or ≥125 nmol/L is commonly used as elevated/risk-enhancing
- Why it matters
- Mostly genetic and can raise lifetime ASCVD/aortic-valve risk
- What changes the plan
- High Lp(a) usually means managing every modifiable risk factor more aggressively
CAC
- Useful anchor
- Most useful in selected borderline/intermediate-risk adults when statin decision is uncertain
- Why it matters
- Shows calcified coronary plaque burden, not total plaque or future immunity
- What changes the plan
- Use when it will change a decision; do not use as a universal reassurance scan
| Signal | Useful anchor | Why it matters | What changes the plan |
|---|---|---|---|
| LDL-C | LDL-C ≥190 mg/dL is a major red flag; lower targets depend on total risk | LDL is a causal atherogenic exposure over time | Very high LDL, premature family history, diabetes, CKD, high 10-year risk, or existing ASCVD shifts intensity |
| Non-HDL-C | Useful when triglycerides are elevated or LDL alone may understate particle burden | Captures cholesterol carried by ApoB-containing particles | Discordance with LDL-C can support checking ApoB and treating the risk stack, not the prettiest number |
| ApoB | ApoB ≥130 mg/dL is often treated as a risk-enhancing signal; lower targets are risk-dependent | Counts atherogenic particles more directly than LDL-C | Especially useful with insulin resistance, high triglycerides, obesity, diabetes risk, or LDL/ApoB discordance |
| Lp(a) | Check once in adulthood; ≥50 mg/dL or ≥125 nmol/L is commonly used as elevated/risk-enhancing | Mostly genetic and can raise lifetime ASCVD/aortic-valve risk | High Lp(a) usually means managing every modifiable risk factor more aggressively |
| CAC | Most useful in selected borderline/intermediate-risk adults when statin decision is uncertain | Shows calcified coronary plaque burden, not total plaque or future immunity | Use when it will change a decision; do not use as a universal reassurance scan |
Lp(a) is mostly genetic. A high value can change how aggressively the rest of the risk stack should be managed. CAC can help selected adults when the statin decision is uncertain. It is not a moral verdict on your arteries.
3. Metabolic risk: glucose, waist, liver, kidney, and insulin-resistance context
Metabolic risk affects cardiovascular disease, kidney disease, fatty liver, sleep apnea, neuropathy, infections, cancer risk patterns, and cognitive aging.
The minimum audit usually includes A1c and/or fasting glucose by age/risk, waist or another visceral-fat proxy when useful, blood pressure, lipids, triglycerides, HDL-C, liver enzymes, and kidney markers when context supports them.
Protocol
Metabolic and organ-risk anchors
A1c
- Typical range or trigger
- Normal <5.7%; prediabetes 5.7–6.4%; diabetes ≥6.5%
- What it catches
- Average glycemia over roughly 2–3 months; imperfect with anemia, hemoglobin variants, pregnancy, CKD, and some ethnic/genetic contexts
- Next move
- If prediabetes or diabetes range, confirm and build a plan; do not “watch” it for years without intervention
Fasting glucose
- Typical range or trigger
- Normal <100 mg/dL; impaired fasting glucose 100–125; diabetes-range ≥126
- What it catches
- Fasting hepatic glucose output and insulin-resistance context
- Next move
- Repeat/confirm abnormal results; pair with A1c, triglycerides, waist, BP, and family history
Triglycerides / HDL-C
- Typical range or trigger
- TG ≥150 mg/dL is a common risk flag; low HDL is context, not a drug target by itself
- What it catches
- Often tracks insulin resistance, alcohol effect, thyroid, genetics, medications, and liver fat
- Next move
- Look for the pattern: waist, A1c/glucose, ApoB, alcohol, diet quality, sleep apnea, liver enzymes
Waist circumference
- Typical range or trigger
- >35 in women or >40 in men is a traditional cardiometabolic-risk threshold; ethnicity-specific thresholds may be lower
- What it catches
- Visceral adiposity proxy; more informative than BMI alone for many people
- Next move
- Measure consistently; use it with labs and blood pressure, not as a shame metric
Liver enzymes / fatty liver context
- Typical range or trigger
- Persistent ALT/AST elevation, metabolic risk, alcohol, viral hepatitis risk, or steatotic liver disease history
- What it catches
- Liver disease can be silent until late
- Next move
- Review alcohol, metabolic risk, medications/supplements, hepatitis testing, fibrosis risk, and imaging only when useful
Kidney markers
- Typical range or trigger
- Creatinine/eGFR plus urine albumin-creatinine ratio in higher-risk people
- What it catches
- Kidney risk is easy to miss if you only look at creatinine
- Next move
- Prioritize if diabetes, hypertension, ASCVD, autoimmune disease, family history, pregnancy complications, or nephrotoxic medication exposure
| Signal | Typical range or trigger | What it catches | Next move |
|---|---|---|---|
| A1c | Normal <5.7%; prediabetes 5.7–6.4%; diabetes ≥6.5% | Average glycemia over roughly 2–3 months; imperfect with anemia, hemoglobin variants, pregnancy, CKD, and some ethnic/genetic contexts | If prediabetes or diabetes range, confirm and build a plan; do not “watch” it for years without intervention |
| Fasting glucose | Normal <100 mg/dL; impaired fasting glucose 100–125; diabetes-range ≥126 | Fasting hepatic glucose output and insulin-resistance context | Repeat/confirm abnormal results; pair with A1c, triglycerides, waist, BP, and family history |
| Triglycerides / HDL-C | TG ≥150 mg/dL is a common risk flag; low HDL is context, not a drug target by itself | Often tracks insulin resistance, alcohol effect, thyroid, genetics, medications, and liver fat | Look for the pattern: waist, A1c/glucose, ApoB, alcohol, diet quality, sleep apnea, liver enzymes |
| Waist circumference | >35 in women or >40 in men is a traditional cardiometabolic-risk threshold; ethnicity-specific thresholds may be lower | Visceral adiposity proxy; more informative than BMI alone for many people | Measure consistently; use it with labs and blood pressure, not as a shame metric |
| Liver enzymes / fatty liver context | Persistent ALT/AST elevation, metabolic risk, alcohol, viral hepatitis risk, or steatotic liver disease history | Liver disease can be silent until late | Review alcohol, metabolic risk, medications/supplements, hepatitis testing, fibrosis risk, and imaging only when useful |
| Kidney markers | Creatinine/eGFR plus urine albumin-creatinine ratio in higher-risk people | Kidney risk is easy to miss if you only look at creatinine | Prioritize if diabetes, hypertension, ASCVD, autoimmune disease, family history, pregnancy complications, or nephrotoxic medication exposure |
The USPSTF recommends screening adults 35 to 70 with overweight or obesity for prediabetes and type 2 diabetes, with individualized earlier screening for higher-risk histories. If prediabetes is found, it is not a shrug: the Diabetes Prevention Program showed intensive lifestyle intervention reduced diabetes incidence by 58 percent compared with placebo over about 2.8 years, with metformin reducing incidence by 31 percent.
4. Cancer and preventive screening: right test, right person, right interval
Cancer screening is not “scan everything and hope.” It is the right test, for the right risk, at the right interval, with a plan for what happens if the result is abnormal. That includes standard screening first, and it can include emerging tools when the consent and follow-up plan are mature enough.
Protocol
Screening loops most adults should audit
Colorectal cancer
- Common evidence-based anchor
- Average-risk adults generally start at 45; routine screening usually through 75
- Who needs personalization
- Family history, prior polyps, inflammatory bowel disease, hereditary syndromes, symptoms
- Open-loop question
- Am I up to date, and if I used stool testing, was any positive result followed by colonoscopy?
Breast cancer
- Common evidence-based anchor
- USPSTF: mammogram every 2 years from 40 to 74 for average-risk women
- Who needs personalization
- Dense breasts, prior atypia, chest radiation, strong family history, BRCA/Lynch-related patterns
- Open-loop question
- Is my interval/risk category explicit rather than inherited from a generic reminder?
Cervical cancer
- Common evidence-based anchor
- Age 21–65 using cytology/HPV strategy by age and history
- Who needs personalization
- Prior abnormal results, immunosuppression, DES exposure, hysterectomy details
- Open-loop question
- Do I know my last Pap/HPV result and the actual follow-up interval?
Lung cancer
- Common evidence-based anchor
- Annual low-dose CT for adults 50–80 with ≥20 pack-years who currently smoke or quit within 15 years
- Who needs personalization
- Occupational exposures, symptoms, prior nodules, comorbidities that affect treatment candidacy
- Open-loop question
- If I qualify, am I in a structured screening program with follow-up?
Prostate cancer
- Common evidence-based anchor
- Shared decision-making is commonly emphasized for men 55–69
- Who needs personalization
- Black ancestry, strong family history, BRCA2 or other hereditary risk, urinary symptoms
- Open-loop question
- Was PSA ordered as a decision or as a reflex? What would we do with the result?
Skin cancer
- Common evidence-based anchor
- Risk-based skin exams rather than universal population screening
- Who needs personalization
- Personal or family history, many atypical nevi, immunosuppression, high UV exposure, prior skin cancer
- Open-loop question
- Should I have a dermatologist skin check interval, and do I know what changes should trigger a visit?
MCED blood tests
- Common evidence-based anchor
- Emerging and promising; not a replacement for standard screening or a proven mortality-reduction tool yet
- Who needs personalization
- Best considered when the person understands false positives, false negatives, uncertain benefit, follow-up testing, cost, and anxiety burden
- Open-loop question
- Would this result change my plan, and do we have a concrete diagnostic pathway if it is positive?
Whole-body MRI
- Common evidence-based anchor
- Emerging adjunct for selected, well-counseled people; especially different from casual “scan everything” marketing
- Who needs personalization
- Can detect some unexpected findings without radiation, but incidental findings and follow-up cascades are common and mortality benefit is unproven
- Open-loop question
- Who reads it, what protocol is used, what findings will we ignore, and who owns follow-up?
Hepatitis C
- Common evidence-based anchor
- USPSTF: adults 18–79; CDC: all adults at least once, plus each pregnancy and periodic testing for ongoing risk
- Who needs personalization
- Injection drug use, HIV, dialysis, abnormal liver tests, transfusion before 1992
- Open-loop question
- Was a positive antibody followed by RNA testing?
AAA
- Common evidence-based anchor
- One-time ultrasound for men 65–75 who have ever smoked; selective decisions for others
- Who needs personalization
- Family history, connective-tissue disease, sex-specific uncertainty
- Open-loop question
- Do I actually meet criteria, or am I imaging because “more screening” feels safer?
Osteoporosis
- Common evidence-based anchor
- Women ≥65 and younger postmenopausal women at increased risk
- Who needs personalization
- Steroids, early menopause, low-trauma fracture, low BMI, parental hip fracture, aromatase inhibitors, malabsorption
- Open-loop question
- Am I evaluating fracture risk, not just admiring a body-composition DXA?
| Screening area | Common evidence-based anchor | Who needs personalization | Open-loop question |
|---|---|---|---|
| Colorectal cancer | Average-risk adults generally start at 45; routine screening usually through 75 | Family history, prior polyps, inflammatory bowel disease, hereditary syndromes, symptoms | Am I up to date, and if I used stool testing, was any positive result followed by colonoscopy? |
| Breast cancer | USPSTF: mammogram every 2 years from 40 to 74 for average-risk women | Dense breasts, prior atypia, chest radiation, strong family history, BRCA/Lynch-related patterns | Is my interval/risk category explicit rather than inherited from a generic reminder? |
| Cervical cancer | Age 21–65 using cytology/HPV strategy by age and history | Prior abnormal results, immunosuppression, DES exposure, hysterectomy details | Do I know my last Pap/HPV result and the actual follow-up interval? |
| Lung cancer | Annual low-dose CT for adults 50–80 with ≥20 pack-years who currently smoke or quit within 15 years | Occupational exposures, symptoms, prior nodules, comorbidities that affect treatment candidacy | If I qualify, am I in a structured screening program with follow-up? |
| Prostate cancer | Shared decision-making is commonly emphasized for men 55–69 | Black ancestry, strong family history, BRCA2 or other hereditary risk, urinary symptoms | Was PSA ordered as a decision or as a reflex? What would we do with the result? |
| Skin cancer | Risk-based skin exams rather than universal population screening | Personal or family history, many atypical nevi, immunosuppression, high UV exposure, prior skin cancer | Should I have a dermatologist skin check interval, and do I know what changes should trigger a visit? |
| MCED blood tests | Emerging and promising; not a replacement for standard screening or a proven mortality-reduction tool yet | Best considered when the person understands false positives, false negatives, uncertain benefit, follow-up testing, cost, and anxiety burden | Would this result change my plan, and do we have a concrete diagnostic pathway if it is positive? |
| Whole-body MRI | Emerging adjunct for selected, well-counseled people; especially different from casual “scan everything” marketing | Can detect some unexpected findings without radiation, but incidental findings and follow-up cascades are common and mortality benefit is unproven | Who reads it, what protocol is used, what findings will we ignore, and who owns follow-up? |
| Hepatitis C | USPSTF: adults 18–79; CDC: all adults at least once, plus each pregnancy and periodic testing for ongoing risk | Injection drug use, HIV, dialysis, abnormal liver tests, transfusion before 1992 | Was a positive antibody followed by RNA testing? |
| AAA | One-time ultrasound for men 65–75 who have ever smoked; selective decisions for others | Family history, connective-tissue disease, sex-specific uncertainty | Do I actually meet criteria, or am I imaging because “more screening” feels safer? |
| Osteoporosis | Women ≥65 and younger postmenopausal women at increased risk | Steroids, early menopause, low-trauma fracture, low BMI, parental hip fracture, aromatase inhibitors, malabsorption | Am I evaluating fracture risk, not just admiring a body-composition DXA? |
The point is screening with follow-through. MCED blood tests and whole-body MRI are emerging and promising, and I think they can be worth doing for the right person. But they are not magic shields or replacements for colonoscopy, mammography, cervical screening, lung screening when eligible, or risk-based workups. The consent has to be honest: false positives, false negatives, incidental findings, downstream imaging/biopsy, anxiety, cost, insurance friction, and still-uncertain mortality benefit.
5. Sleep apnea: do not normalize low oxygen and broken sleep
Sleep apnea is a fatal-loop issue when the history fits: loud snoring, witnessed apneas, morning headaches, resistant hypertension, atrial fibrillation, unexplained fatigue, reflux, nocturia, or high-risk anatomy. It affects blood pressure, arrhythmia risk, metabolic control, mood, cognition, and accident risk.
The audit question is not “am I tired?” It is “is my sleep fragmenting my physiology enough that testing and treatment would change the plan?” Home sleep apnea testing or polysomnography belongs here when the pre-test probability is real.
6. Kidney, liver, and selective vascular screening
Kidney and liver disease often sit behind more glamorous risks. For kidney risk, the basics are creatinine/eGFR and urine albumin-creatinine ratio in people with diabetes, hypertension, cardiovascular disease, prior abnormal kidney labs, family history, pregnancy complications, autoimmune disease, or nephrotoxic medication exposure.
For liver risk, ask about alcohol, metabolic risk, viral hepatitis, medications, supplements, and persistent liver enzyme abnormalities. For aneurysms, be targeted: AAA ultrasound where indicated, and brain aneurysm screening only in high-risk contexts such as multiple affected first-degree relatives, ADPKD, or selected genetic syndromes.
A good audit is not “image everything.” It is “screen where finding something is likely to help, and use broader tools only when the person understands what may happen next.”
Tier 2: remove asymmetric risks
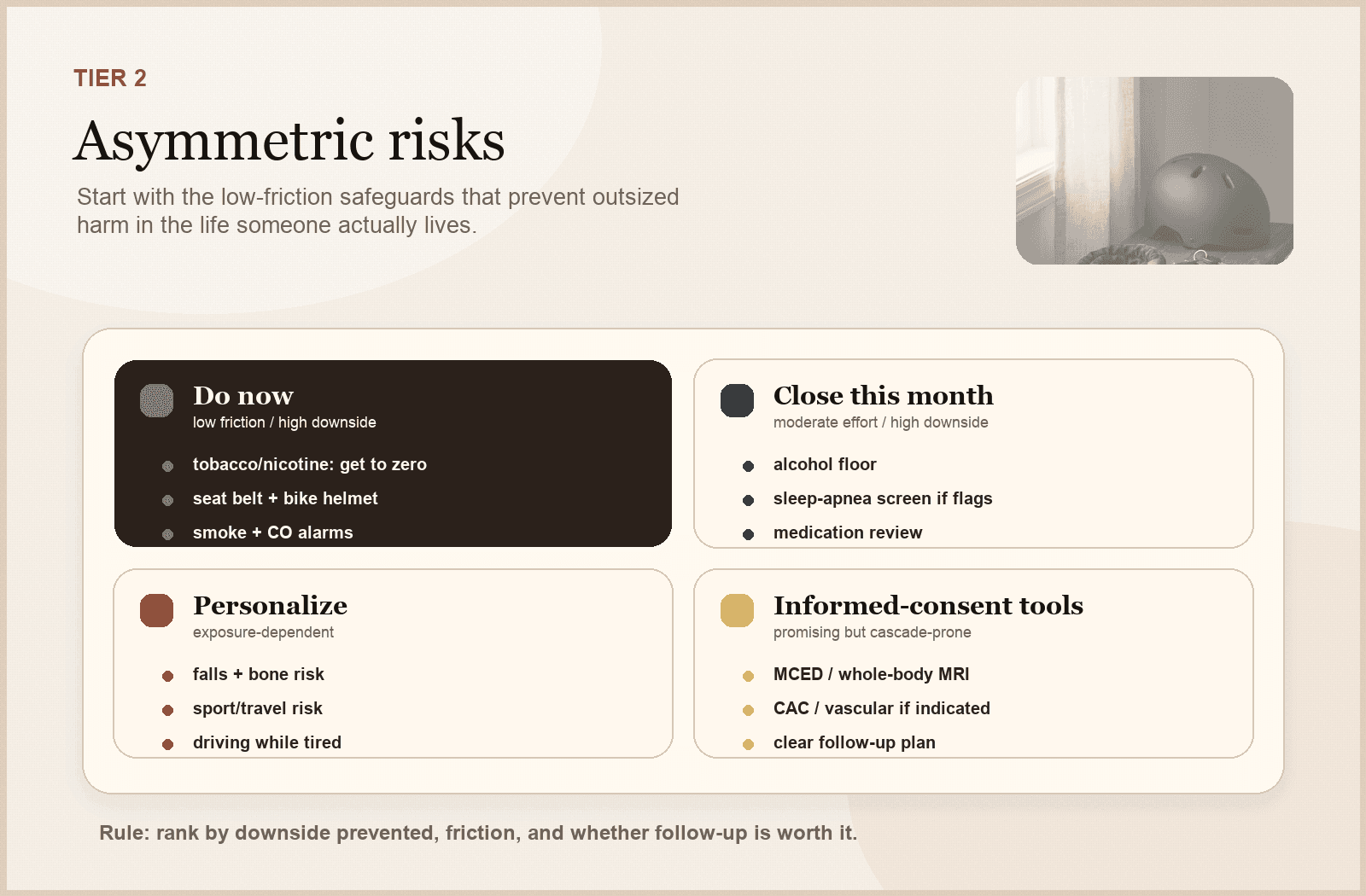
Low-friction safeguards can outrank glamorous optimization when the downside prevented is large.
Some risks are obvious enough that longevity people skip them. That is a mistake. This is where tobacco/nicotine exposure belongs: not because it is small, but because the intervention logic is asymmetric.
Tobacco, nicotine, and smoke exposure
Combustible tobacco is one of the clearest asymmetric risks in medicine: huge downside, strong evidence, and a concrete first decision—get exposure to zero with real support. Vaping, nicotine pouches, and secondhand smoke are not identical to cigarettes, but they still belong in the audit because they can reinforce dependence, affect blood pressure and sleep, and change lung-screening or vascular-risk context.
This should not be handled as a moral lecture or a checkbox. It should be handled as a system: identify the exposure, reduce friction, use evidence-based cessation tools when needed, and make sure anyone who qualifies for lung cancer screening is actually in a structured follow-up pathway.
Protocol
Asymmetric risk anchors
Tobacco / nicotine exposure
- Anchor
- Combustible tobacco: get to zero. Vaping, pouches, and secondhand smoke still belong in the audit because dependence, BP/sympathetic tone, sleep, anxiety, and lung-screening eligibility can matter.
- Why it matters
- Very large downside relative to the first decision: identify exposure, reduce friction, and use evidence-based support rather than willpower theater.
- Audit move
- Ask about smoking, vaping, nicotine pouches, secondhand exposure, cessation meds/coaching, and whether lung cancer screening criteria are met.
Alcohol
- Anchor
- Binge drinking: ≥4 drinks for women or ≥5 for men on an occasion. Heavy drinking: ≥8 drinks/week for women or ≥15 for men.
- Why it matters
- Alcohol worsens sleep, BP, AFib risk, liver disease, injury risk, reflux, mood, cancer risk, cravings, and medication interactions.
- Audit move
- Track actual weekly pattern and run a lower-intake experiment if sleep, BP, HRV/RHR, mood, reflux, or cravings worsen after drinking.
Seat belts
- Anchor
- Front-seat belts cut fatal-injury risk roughly in half in passenger vehicles.
- Why it matters
- A one-second habit prevents a catastrophic tail risk.
- Audit move
- Every trip, every seat; especially taxis/rideshare/late nights.
Helmets / exposure safety
- Anchor
- Risk depends on actual exposure: bikes, e-bikes, skiing, motorcycles, climbing, commuting while sleep-deprived.
- Why it matters
- Asymmetric risk math beats aesthetic objections.
- Audit move
- Match the safeguard to the activity you actually do.
Falls and fractures
- Anchor
- Adults ≥65 at increased fall risk benefit from exercise interventions; osteoporosis screening matters by age/risk.
- Why it matters
- Falls can collapse independence quickly.
- Audit move
- Review falls/near-falls, balance, vision/hearing, sedating meds, footwear, strength, and DXA/fracture-risk context.
Medication burden
- Anchor
- Benzodiazepines, Z-drugs, opioids, gabapentinoids, anticholinergics, NSAIDs, PPIs, duplicates, and supplements can add hidden risk.
- Why it matters
- Side effects masquerade as aging.
- Audit move
- Bring the real list, including supplements, and ask what can be simplified safely.
Vaccines
- Anchor
- CDC adult schedule changes by age, risk, pregnancy, immune status, and prior doses.
- Why it matters
- Low-drama prevention for high-cost infections.
- Audit move
- Audit flu, COVID, Tdap/Td, shingles, pneumococcal, RSV, hepatitis B, travel, and risk-based vaccines.
Aspirin
- Anchor
- USPSTF: individual decision age 40–59 with ≥10% 10-year CVD risk; do not initiate for primary prevention at ≥60.
- Why it matters
- Prevention can harm when bleeding risk exceeds benefit.
- Audit move
- Do not start or stop casually; review indication, age, bleeding risk, and CVD risk with a clinician.
| Area | Anchor | Why it matters | Audit move |
|---|---|---|---|
| Tobacco / nicotine exposure | Combustible tobacco: get to zero. Vaping, pouches, and secondhand smoke still belong in the audit because dependence, BP/sympathetic tone, sleep, anxiety, and lung-screening eligibility can matter. | Very large downside relative to the first decision: identify exposure, reduce friction, and use evidence-based support rather than willpower theater. | Ask about smoking, vaping, nicotine pouches, secondhand exposure, cessation meds/coaching, and whether lung cancer screening criteria are met. |
| Alcohol | Binge drinking: ≥4 drinks for women or ≥5 for men on an occasion. Heavy drinking: ≥8 drinks/week for women or ≥15 for men. | Alcohol worsens sleep, BP, AFib risk, liver disease, injury risk, reflux, mood, cancer risk, cravings, and medication interactions. | Track actual weekly pattern and run a lower-intake experiment if sleep, BP, HRV/RHR, mood, reflux, or cravings worsen after drinking. |
| Seat belts | Front-seat belts cut fatal-injury risk roughly in half in passenger vehicles. | A one-second habit prevents a catastrophic tail risk. | Every trip, every seat; especially taxis/rideshare/late nights. |
| Helmets / exposure safety | Risk depends on actual exposure: bikes, e-bikes, skiing, motorcycles, climbing, commuting while sleep-deprived. | Asymmetric risk math beats aesthetic objections. | Match the safeguard to the activity you actually do. |
| Falls and fractures | Adults ≥65 at increased fall risk benefit from exercise interventions; osteoporosis screening matters by age/risk. | Falls can collapse independence quickly. | Review falls/near-falls, balance, vision/hearing, sedating meds, footwear, strength, and DXA/fracture-risk context. |
| Medication burden | Benzodiazepines, Z-drugs, opioids, gabapentinoids, anticholinergics, NSAIDs, PPIs, duplicates, and supplements can add hidden risk. | Side effects masquerade as aging. | Bring the real list, including supplements, and ask what can be simplified safely. |
| Vaccines | CDC adult schedule changes by age, risk, pregnancy, immune status, and prior doses. | Low-drama prevention for high-cost infections. | Audit flu, COVID, Tdap/Td, shingles, pneumococcal, RSV, hepatitis B, travel, and risk-based vaccines. |
| Aspirin | USPSTF: individual decision age 40–59 with ≥10% 10-year CVD risk; do not initiate for primary prevention at ≥60. | Prevention can harm when bleeding risk exceeds benefit. | Do not start or stop casually; review indication, age, bleeding risk, and CVD risk with a clinician. |
Alcohol is not a longevity supplement with a branding problem. Tobacco and nicotine exposure do not become harmless because the delivery device looks modern. Seat belts and helmets are not wellness content, but they may beat half the supplement aisle on downside prevented.
Tier 3: build physiologic reserve
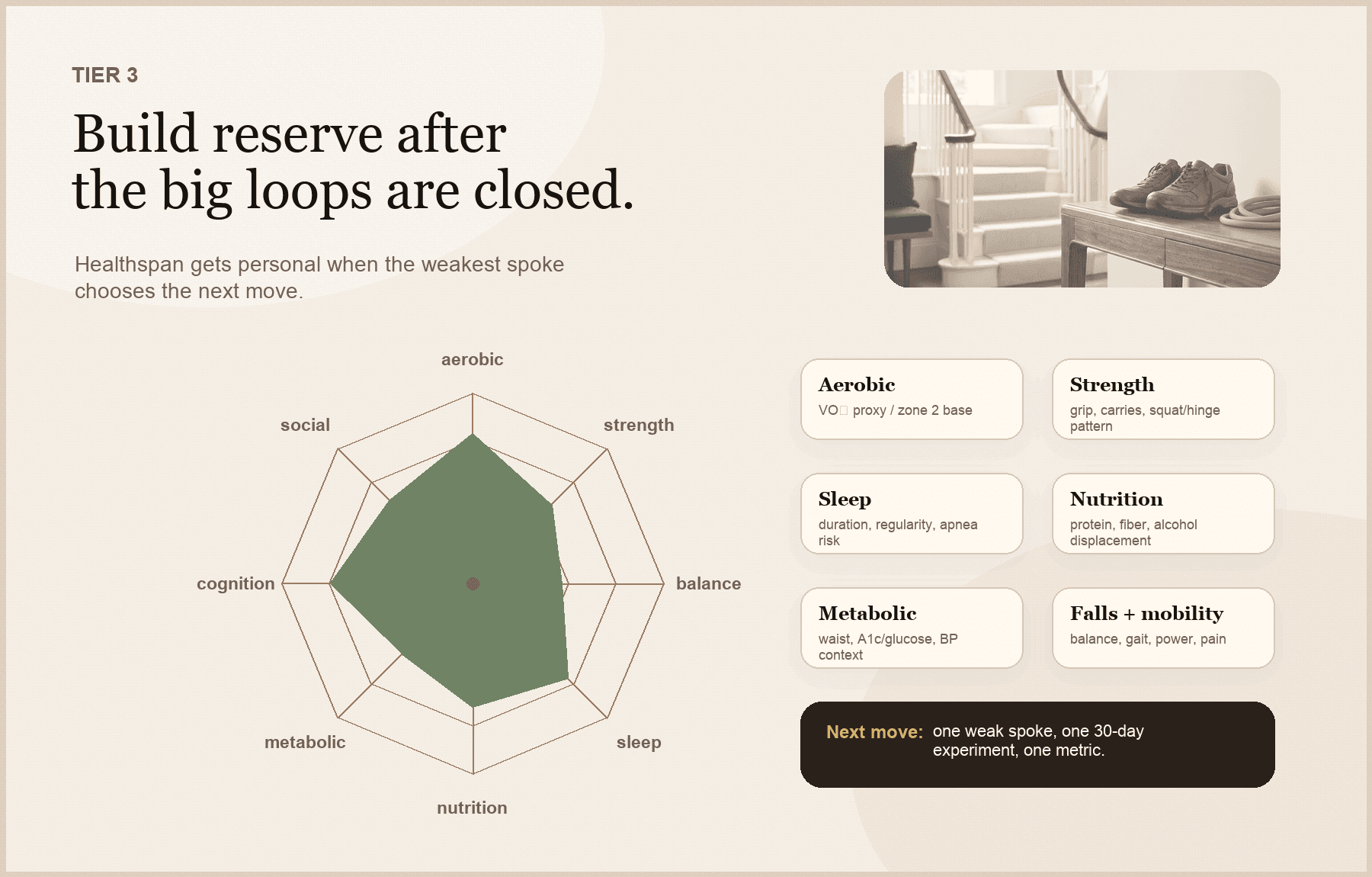
Healthspan work becomes personal when the weakest spoke chooses the next move.
Closing fatal loops helps you avoid preventable disease. Building reserve helps you stay functional when life happens.
Protocol
Physiologic reserve targets
Cardiorespiratory fitness
- Practical anchor
- At least 150 min/week moderate activity, 75 min/week vigorous, or a mix; more helps if recovered well
- What it tells you
- Integrates heart, lungs, vessels, muscle, mitochondria, autonomic tone, and behavior
- First move
- Build a floor first: walking, cycling, incline, zone 2-ish work, then safe intensity if appropriate
Strength
- Practical anchor
- Muscle-strengthening activity at least 2 days/week, all major muscle groups
- What it tells you
- Predicts function: stairs, luggage, illness recovery, falls, independence
- First move
- Two full-body sessions beat a perfect plan you never start
Balance / power
- Practical anchor
- Especially important with age, falls, vestibular issues, neuropathy, sedating meds, or low activity
- What it tells you
- Fall risk is often trainable
- First move
- Single-leg stance, sit-to-stand, carries, stepping, supervised balance/physical therapy if risk is high
Nutrition
- Practical anchor
- Fiber around 25–29 g/day is a useful evidence-backed anchor; protein depends on age, training, weight loss, and frailty risk
- What it tells you
- Diet should move physiology: ApoB, BP, A1c, liver enzymes, waist, satiety, digestion, muscle
- First move
- Add fiber/protein before adding rules; use labs and function as feedback
Sleep
- Practical anchor
- Adults generally need 7+ hours; 61–64: 7–9; 65+: 7–8 is a common range
- What it tells you
- Sleep affects BP, glycemia, appetite, mood, cognition, pain, injury risk, and recovery
- First move
- Protect schedule and screen for apnea symptoms: snoring, witnessed apneas, gasping, morning headaches, sleepiness, resistant hypertension, AFib
Social / sensory
- Practical anchor
- Recurring contact, hearing and vision correction when needed, crisis support
- What it tells you
- Isolation, hearing loss, vision loss, depression, and caregiver strain can become health risks
- First move
- Make it operational: who, when, how often, and what ritual keeps it alive
| Domain | Practical anchor | What it tells you | First move |
|---|---|---|---|
| Cardiorespiratory fitness | At least 150 min/week moderate activity, 75 min/week vigorous, or a mix; more helps if recovered well | Integrates heart, lungs, vessels, muscle, mitochondria, autonomic tone, and behavior | Build a floor first: walking, cycling, incline, zone 2-ish work, then safe intensity if appropriate |
| Strength | Muscle-strengthening activity at least 2 days/week, all major muscle groups | Predicts function: stairs, luggage, illness recovery, falls, independence | Two full-body sessions beat a perfect plan you never start |
| Balance / power | Especially important with age, falls, vestibular issues, neuropathy, sedating meds, or low activity | Fall risk is often trainable | Single-leg stance, sit-to-stand, carries, stepping, supervised balance/physical therapy if risk is high |
| Nutrition | Fiber around 25–29 g/day is a useful evidence-backed anchor; protein depends on age, training, weight loss, and frailty risk | Diet should move physiology: ApoB, BP, A1c, liver enzymes, waist, satiety, digestion, muscle | Add fiber/protein before adding rules; use labs and function as feedback |
| Sleep | Adults generally need 7+ hours; 61–64: 7–9; 65+: 7–8 is a common range | Sleep affects BP, glycemia, appetite, mood, cognition, pain, injury risk, and recovery | Protect schedule and screen for apnea symptoms: snoring, witnessed apneas, gasping, morning headaches, sleepiness, resistant hypertension, AFib |
| Social / sensory | Recurring contact, hearing and vision correction when needed, crisis support | Isolation, hearing loss, vision loss, depression, and caregiver strain can become health risks | Make it operational: who, when, how often, and what ritual keeps it alive |
If I could only know one “longevity lab” about someone, I would rather know how much work their body can do than how many supplements they take.
Hormone health belongs, but not as a generic panel
Hormones belong in a longevity audit because transitions can change sleep, mood, bone, muscle, sexual function, fertility, cardiometabolic risk, and day-to-day function. They do not belong as a generic “optimize your hormones” panel for everyone with a credit card.
Protocol
When hormones become audit-relevant
Menstrual / reproductive
- What to look for
- Irregular cycles, amenorrhea, heavy bleeding, infertility, PCOS, hyperandrogenic symptoms, low-energy availability
- Why it matters
- Can signal endocrine, metabolic, bone, or fertility issues
- Caution
- Do not reduce it to a random day-3 panel without a question
Pregnancy history
- What to look for
- Gestational diabetes, preeclampsia, gestational hypertension, preterm birth, recurrent pregnancy loss
- Why it matters
- Changes long-term cardiometabolic risk assessment
- Caution
- Pregnancy complications are not “old history” for prevention
Perimenopause / menopause
- What to look for
- Vasomotor symptoms, sleep disruption, genitourinary symptoms, early menopause/POI, surgical menopause, bone risk, abnormal bleeding
- Why it matters
- Symptoms, bone, cardiometabolic shifts, and quality of life may change the plan
- Caution
- MHT can be appropriate for symptoms/risk context, but not generic chronic-disease prevention
Testosterone in men
- What to look for
- Low libido, erectile dysfunction, unexplained anemia, low bone density, infertility concerns, loss of muscle/strength in context
- Why it matters
- Diagnosis requires symptoms/signs plus consistently low morning testosterone
- Caution
- One curiosity lab is not a diagnosis
Thyroid
- What to look for
- Palpitations, tremor, heat/cold intolerance, constipation, unexplained weight change, goiter, autoimmune history, lithium/amiodarone
- Why it matters
- Thyroid disease can mimic many “optimization” complaints
- Caution
- Routine asymptomatic screening is not always high-yield; symptoms/risk matter
| Context | What to look for | Why it matters | Caution |
|---|---|---|---|
| Menstrual / reproductive | Irregular cycles, amenorrhea, heavy bleeding, infertility, PCOS, hyperandrogenic symptoms, low-energy availability | Can signal endocrine, metabolic, bone, or fertility issues | Do not reduce it to a random day-3 panel without a question |
| Pregnancy history | Gestational diabetes, preeclampsia, gestational hypertension, preterm birth, recurrent pregnancy loss | Changes long-term cardiometabolic risk assessment | Pregnancy complications are not “old history” for prevention |
| Perimenopause / menopause | Vasomotor symptoms, sleep disruption, genitourinary symptoms, early menopause/POI, surgical menopause, bone risk, abnormal bleeding | Symptoms, bone, cardiometabolic shifts, and quality of life may change the plan | MHT can be appropriate for symptoms/risk context, but not generic chronic-disease prevention |
| Testosterone in men | Low libido, erectile dysfunction, unexplained anemia, low bone density, infertility concerns, loss of muscle/strength in context | Diagnosis requires symptoms/signs plus consistently low morning testosterone | One curiosity lab is not a diagnosis |
| Thyroid | Palpitations, tremor, heat/cold intolerance, constipation, unexplained weight change, goiter, autoimmune history, lithium/amiodarone | Thyroid disease can mimic many “optimization” complaints | Routine asymptomatic screening is not always high-yield; symptoms/risk matter |
Menopausal hormone therapy can be appropriate for symptoms and selected risk contexts, especially near menopause, but it should not be sold as generic chronic-disease prevention. Testosterone diagnosis requires compatible symptoms or signs plus consistently low morning testosterone, not one curiosity lab.
Biomarkers and wearables: use the actionability filter
A biomarker earns its place only when it changes the next decision.
The best biomarker is not the most obscure one. It is the one that changes the next decision.
Protocol
Actionability filter for tests and trackers
If abnormal, what would I do?
- Good answer
- A specific next step: repeat, treat, refer, change behavior, change medication, or stop an exposure
- Weak answer
- I would worry more or buy more tests
- Decision
- Order only if the next step is clear enough
If normal, what would I stop doing?
- Good answer
- It would safely avoid a medication, scan, referral, or repeated monitoring
- Weak answer
- I would still keep checking it
- Decision
- Normal results should reduce noise, not add another dashboard
Is the measurement reliable?
- Good answer
- Validated method, standardized conditions, known limitations
- Weak answer
- Consumer score with unclear validity
- Decision
- Trend only what deserves a trend
Could it cause harm?
- Good answer
- False positives/negatives and incidental findings are understood
- Weak answer
- More data is assumed to be safer
- Decision
- Include cascade risk in the decision
Will tracking improve behavior?
- Good answer
- It changes sleep, activity, nutrition, medication adherence, or follow-up
- Weak answer
- It makes me more obsessive without changing the plan
- Decision
- Actionability beats curiosity
| Question | Good answer | Weak answer | Decision |
|---|---|---|---|
| If abnormal, what would I do? | A specific next step: repeat, treat, refer, change behavior, change medication, or stop an exposure | I would worry more or buy more tests | Order only if the next step is clear enough |
| If normal, what would I stop doing? | It would safely avoid a medication, scan, referral, or repeated monitoring | I would still keep checking it | Normal results should reduce noise, not add another dashboard |
| Is the measurement reliable? | Validated method, standardized conditions, known limitations | Consumer score with unclear validity | Trend only what deserves a trend |
| Could it cause harm? | False positives/negatives and incidental findings are understood | More data is assumed to be safer | Include cascade risk in the decision |
| Will tracking improve behavior? | It changes sleep, activity, nutrition, medication adherence, or follow-up | It makes me more obsessive without changing the plan | Actionability beats curiosity |
High-yield measurements usually include home blood pressure, LDL-C/non-HDL-C/ApoB, Lp(a) once, A1c or fasting glucose by age/risk, waist or body composition when management-changing, eGFR/uACR in higher-risk people, liver enzymes when alcohol/metabolic/medication context supports it, and CBC/ferritin/B12/TSH/vitamin D only when symptoms or risk make them actionable.
Wearables can help with trends: steps, activity minutes, resting heart rate, estimated fitness, sleep duration, sleep regularity, and HRV as a within-person recovery signal. CGM is high-value for diabetes and selected prediabetes, hypoglycemia, or short experiments; it is not a prerequisite before blood pressure, lipids, activity, strength, nutrition, and sleep. Normal wearable data does not rule out disease.
How to personalize the audit
The same checklist should not produce the same order for everyone.
Protocol
Personalization map by age and risk
20s–30s
- What usually moves up
- Baseline BP, lipids, Lp(a), family history, tobacco/alcohol exposure, fitness, sleep, vaccines, mental health, reproductive goals, high-exposure risks
- What not to miss
- Premature ASCVD family history, very high LDL, PCOS, pregnancy plans, biking/driving/sport risk, shift work
40s
- What usually moves up
- Colorectal screening at 45, breast/cervical screening by risk, ASCVD risk, ApoB/Lp(a), metabolic risk, perimenopause, body composition, sleep, selective CAC decisions
- What not to miss
- Blood pressure drift, insulin resistance, alcohol pattern, family cancer syndromes
50s–60s
- What usually moves up
- Lung screening if eligible, prostate shared decision-making, menopause, testosterone symptoms, bone density, sleep apnea, vaccines, alcohol, strength, balance
- What not to miss
- Medication burden, falls, hearing/vision, kidney/liver risk, high-risk family history
65+
- What usually moves up
- Falls, fractures, medication review, hearing, vision, vaccines, frailty, functional strength, cognition, social support, AAA where indicated
- What not to miss
- Sedatives/anticholinergics, isolation, gait change, undernutrition, osteoporosis
Family / reproductive history
- What usually moves up
- Premature ASCVD, sudden death, early cancer, Lynch/BRCA patterns, aneurysm, ADPKD, dementia, familial hypercholesterolemia, high Lp(a), preeclampsia, gestational diabetes, PCOS, early menopause
- What not to miss
- These can change the order more than age alone
| Context | What usually moves up | What not to miss |
|---|---|---|
| 20s–30s | Baseline BP, lipids, Lp(a), family history, tobacco/alcohol exposure, fitness, sleep, vaccines, mental health, reproductive goals, high-exposure risks | Premature ASCVD family history, very high LDL, PCOS, pregnancy plans, biking/driving/sport risk, shift work |
| 40s | Colorectal screening at 45, breast/cervical screening by risk, ASCVD risk, ApoB/Lp(a), metabolic risk, perimenopause, body composition, sleep, selective CAC decisions | Blood pressure drift, insulin resistance, alcohol pattern, family cancer syndromes |
| 50s–60s | Lung screening if eligible, prostate shared decision-making, menopause, testosterone symptoms, bone density, sleep apnea, vaccines, alcohol, strength, balance | Medication burden, falls, hearing/vision, kidney/liver risk, high-risk family history |
| 65+ | Falls, fractures, medication review, hearing, vision, vaccines, frailty, functional strength, cognition, social support, AAA where indicated | Sedatives/anticholinergics, isolation, gait change, undernutrition, osteoporosis |
| Family / reproductive history | Premature ASCVD, sudden death, early cancer, Lynch/BRCA patterns, aneurysm, ADPKD, dementia, familial hypercholesterolemia, high Lp(a), preeclampsia, gestational diabetes, PCOS, early menopause | These can change the order more than age alone |
The point is not to build a larger checklist. It is to put the right thing first for the person in front of you.
A simple 30-day longevity audit
Do not overhaul your entire life in one weekend. That is how you create a spreadsheet and then avoid it forever.
Protocol
30-day audit plan
Week 1
- Job
- Collect the facts
- Concrete output
- Home BP average, medication/supplement list, recent lipids/ApoB/Lp(a), A1c/glucose, screening dates, vaccines, smoking/alcohol, sleep, steps/exercise, strength, falls history, family history
Week 2
- Job
- Close overdue loops
- Concrete output
- Schedule overdue screening, follow up abnormal results, confirm high BP properly, ask whether ApoB, Lp(a), CAC, uACR, DXA, HCV, or genetic counseling would change the plan
Week 3
- Job
- Install two behaviors
- Concrete output
- Validated BP tracking, two resistance sessions, higher fiber, a higher step floor, a lower-alcohol experiment, a consistent sleep window, or hearing/vision/fall-risk evaluation if relevant
Week 4
- Job
- Run one experiment
- Concrete output
- One question, one intervention, one metric, one decision. Good: increase fiber from 12 to 28 g/day for 8 weeks. Bad: start 12 supplements and see if you feel optimized.
| Week | Job | Concrete output |
|---|---|---|
| Week 1 | Collect the facts | Home BP average, medication/supplement list, recent lipids/ApoB/Lp(a), A1c/glucose, screening dates, vaccines, smoking/alcohol, sleep, steps/exercise, strength, falls history, family history |
| Week 2 | Close overdue loops | Schedule overdue screening, follow up abnormal results, confirm high BP properly, ask whether ApoB, Lp(a), CAC, uACR, DXA, HCV, or genetic counseling would change the plan |
| Week 3 | Install two behaviors | Validated BP tracking, two resistance sessions, higher fiber, a higher step floor, a lower-alcohol experiment, a consistent sleep window, or hearing/vision/fall-risk evaluation if relevant |
| Week 4 | Run one experiment | One question, one intervention, one metric, one decision. Good: increase fiber from 12 to 28 g/day for 8 weeks. Bad: start 12 supplements and see if you feel optimized. |
What not to chase first
Lower priority does not mean never. It means not first.
- Whole-body MRI with no pre-test counseling, no radiology quality standard, and no follow-up plan.
- Broad tumor-marker panels marketed as a shortcut. MCED is different and promising, but still emerging and not a replacement for standard screening.
- Biological-age clocks.
- Generic hormone panels without symptoms or risk context.
- Microbiome reports that do not change the plan.
- CGM for metabolically healthy people before basics are handled.
- CAC as a universal scan.
- Brain aneurysm screening without high-risk context.
- Supplement stacks before BP, lipids, tobacco/nicotine exposure, alcohol, sleep, strength, and screening.
A good audit is not ascetic. It is ordered.
What to ask your clinician
Bring this as a starter list:
- What is my highest-priority preventable risk right now?
- Is my blood pressure actually controlled based on home or ambulatory data?
- Do my lipids, ApoB, Lp(a), family history, or risk enhancers change my ASCVD plan?
- Am I due for colorectal, breast, cervical, lung, prostate, skin, AAA, HCV, or osteoporosis screening based on my age and risk—and would MCED or whole-body MRI add useful information for me specifically?
If I choose MCED or whole-body MRI, what exactly would we do with a positive, negative, or indeterminate result?
- Do my pregnancy history, PCOS, menopause status, testosterone symptoms, thyroid symptoms, or bone risk change what we should check?
- Do any medications or supplements increase my falls, bleeding, kidney, liver, cognition, or sleep risk?
- Which vaccines am I due for under current CDC guidance?
- What result would change management, and what would we do if it is abnormal?
That last question may be the most important one.
Dr. Hillary Lin’s take
Longevity is not doing everything. It is doing the highest-leverage thing in the right order.
I am not against advanced testing. I am more open than many standard checklists to MCED blood tests and whole-body MRI for the right person, because early detection can matter. But I am against pretending they are magic. They need informed consent, a clean follow-up pathway, and the basics handled first.
The boring loops are boring because they have enough evidence to deserve priority. The emerging tools are interesting because they may catch what routine screening misses. Both can be true.
Close warning lights first. Use standard screening, asymmetric safeguards, and reserve-building as the base. Then add advanced tools when the result would actually change the next decision.
Clinical lens
How I’d decide
Use this section as a second pass after the main answer, not as homework before you know what the page is saying.
Who it’s for
Adults who want a practical prevention-first review of longevity risk: especially if they have not recently checked home blood pressure, ApoB/LDL/Lp(a), metabolic risk, cancer screening status, vaccines, alcohol pattern, sleep, fitness, medications, or family-history risk.
Who should skip it
Do not use this as a substitute for evaluation of symptoms, known abnormal results, pregnancy/postpartum concerns, active cancer workups, severe depression or suicidal thoughts, eating-disorder recovery, or complex medical decisions that need clinician context.
Measure before / after
Start with home blood pressure, medications/supplements, tobacco/nicotine and alcohol exposure, LDL-C/non-HDL-C and ApoB when useful, Lp(a) once, A1c or fasting glucose by age/risk, waist or body composition when actionable, kidney/liver markers when risk supports it, screening dates, vaccines, sleep apnea clues, activity, strength, balance, and family history. If considering MCED or whole-body MRI, measure the follow-up plan before the test: who interprets it, what counts as actionable, and what happens next.
What I’d do first
I would first close any abnormal-result or symptom loop, then confirm blood pressure, clarify ApoB/LDL/Lp(a) and metabolic risk, update standard screening, review tobacco/nicotine, alcohol, medications, vaccines, and safety risks, and build two reserve behaviors. Then I would discuss MCED or whole-body MRI only if the person understands the tradeoffs and the result would change care.
What would change my mind
A strong family history, premature ASCVD, very high LDL-C or Lp(a), pregnancy complications, PCOS, early menopause, diabetes, CKD, smoking history, abnormal screening result, falls, frailty, symptoms, medication risk, or a well-counseled decision to use MCED/whole-body MRI can change the order. An advanced test earns a place only if it changes the plan and has a follow-up path.
Frequently Asked Questions
What is a longevity audit?
A prioritized preventive health review. It ranks actions by absolute risk, preventability, actionability, evidence quality, and personalization instead of novelty.
Where do the hallmarks of aging fit?
They are the mechanism map, not the to-do list. Aging biology matters most when it translates into human, measurable, action-changing proxies.
What should I check first for longevity?
Red-flag symptoms and known abnormal results first. Then blood pressure, cardiovascular risk, tobacco, metabolic risk, age and risk appropriate cancer screening, alcohol, medications, vaccines, fitness, strength, sleep, nutrition, and family history.
Are biomarkers useful for longevity?
Yes, when they change decisions. Home blood pressure, ApoB or LDL-C/non-HDL-C, Lp(a) once, A1c or fasting glucose, eGFR/uACR in risk groups, and DXA when indicated can be high-yield. Broad panels can create noise.
Should I get a whole-body MRI?
Not as the first step for most people. It can find incidental findings and miss other risks. It should not outrank evidence-based screening, blood pressure, lipids, smoking, alcohol, metabolic risk, and cancer screening loops.
Should everyone get hormone testing?
No. Hormone evaluation is most useful when symptoms, transitions, fertility goals, bone risk, menstrual changes, menopause, PCOS, testosterone-deficiency symptoms, thyroid symptoms, or medication context make the result actionable.
Is a CGM worth it if I do not have diabetes?
Sometimes, but usually not first. CGM can help with diabetes, prediabetes, suspected hypoglycemia, or a focused short experiment. For metabolically healthy people, BP, lipids, activity, strength, sleep, nutrition, and alcohol often matter more first.
What is the best wearable for longevity?
For many adults, a validated home blood pressure cuff. Step count, sleep regularity, resting heart rate, estimated fitness, and HRV trends can help behavior, but wearables are not diagnostic tests.
How often should I do a longevity audit?
Yearly, or after major changes: new diagnosis, pregnancy/postpartum transition, menopause, new medication, major weight change, family-history discovery, surgery planning, serious illness, or a big training/lifestyle shift.
References & citations
- 1.CDC/NCHS Mortality in the United States, 2023
- 2.GBD 2021 risk factors, Lancet 2024
- 3.Hallmarks of aging: an expanding universe, Cell 2023
- 4.USPSTF hypertension screening
- 5.USPSTF statin primary prevention
- 6.National Lipid Association Lp(a) focused update
- 7.USPSTF prediabetes and type 2 diabetes screening
- 8.Diabetes Prevention Program, NEJM 2002
- 9.USPSTF colorectal cancer screening
- 10.USPSTF breast cancer screening
- 11.USPSTF cervical cancer screening
- 12.USPSTF lung cancer screening
- 13.USPSTF prostate cancer screening
- 14.USPSTF unhealthy alcohol use screening and counseling
- 15.USPSTF tobacco cessation
- 16.USPSTF falls prevention
- 17.USPSTF osteoporosis screening
- 18.CDC adult immunization schedule
- 19.Endocrine Society testosterone therapy guideline
- 20.NAMS 2022 hormone therapy position statement
- 21.USPSTF menopausal hormone therapy for primary prevention
- 22.USPSTF thyroid dysfunction screening
- 23.International Evidence-Based PCOS Guideline 2023
- 24.AHA Life's Essential 8
- 25.Lancet 2019 fiber and carbohydrate quality review
- 26.BMJ/BJSM 2022 muscle-strengthening activity meta-analysis
- 27.PURE grip strength study, Lancet 2015
- 28.Holt-Lunstad social relationships and mortality meta-analysis
- 29.Lancet Commission dementia prevention 2024
- 30.AHA blood pressure categories
- 31.CDC diabetes testing and A1c ranges
- 32.NHLBI waist circumference and healthy weight risk
- 33.CDC alcohol use and health
- 34.CDC hepatitis C testing
- 35.USPSTF aspirin primary prevention
- 36.NHTSA seat belts save lives
- 37.CDC adult physical activity guidelines
- 38.CDC sleep recommendations
- 39.NCI questions and answers about multi-cancer detection tests
- 40.ACR statement on screening total-body MRI
- 41.Whole-body MRI for cancer screening in asymptomatic subjects, review and recommendations
Next step
Turn the guide into the right next decision.
If this page raised a real clinical question, start with the practice details. If you are still learning, get the weekly letter. If you are comparing tests, use the testing hub before buying another panel.