There is no sunblock
How to Choose Sunscreen That Actually Protects You
SPF only rates sunburn. What you need depends on exposure, pigment, texture, and filter quality.
Quick answer+
Choose a broad-spectrum SPF 30+ sunscreen you will actually wear daily. For heavy sun, use SPF 50+, water resistance, enough product, and reapply every two hours. For pigment, use tinted iron oxides; for low systemic uncertainty, use zinc/titanium lotion.
Burn
SPF is only the start
Pigment
Tint covers visible light
Safety
Absorption is not toxicity

Clinical frame
Tint, texture, dose, and reapplication are where most sunscreens fall short.
Photoprotection system
Think in systems, not SPF.
SPF grades one thing: sunburn. UVA, visible light, water and sweat, dose, and reapplication each fail differently. Quick map gives the practical choice. Clinical read shows the mechanism and source.
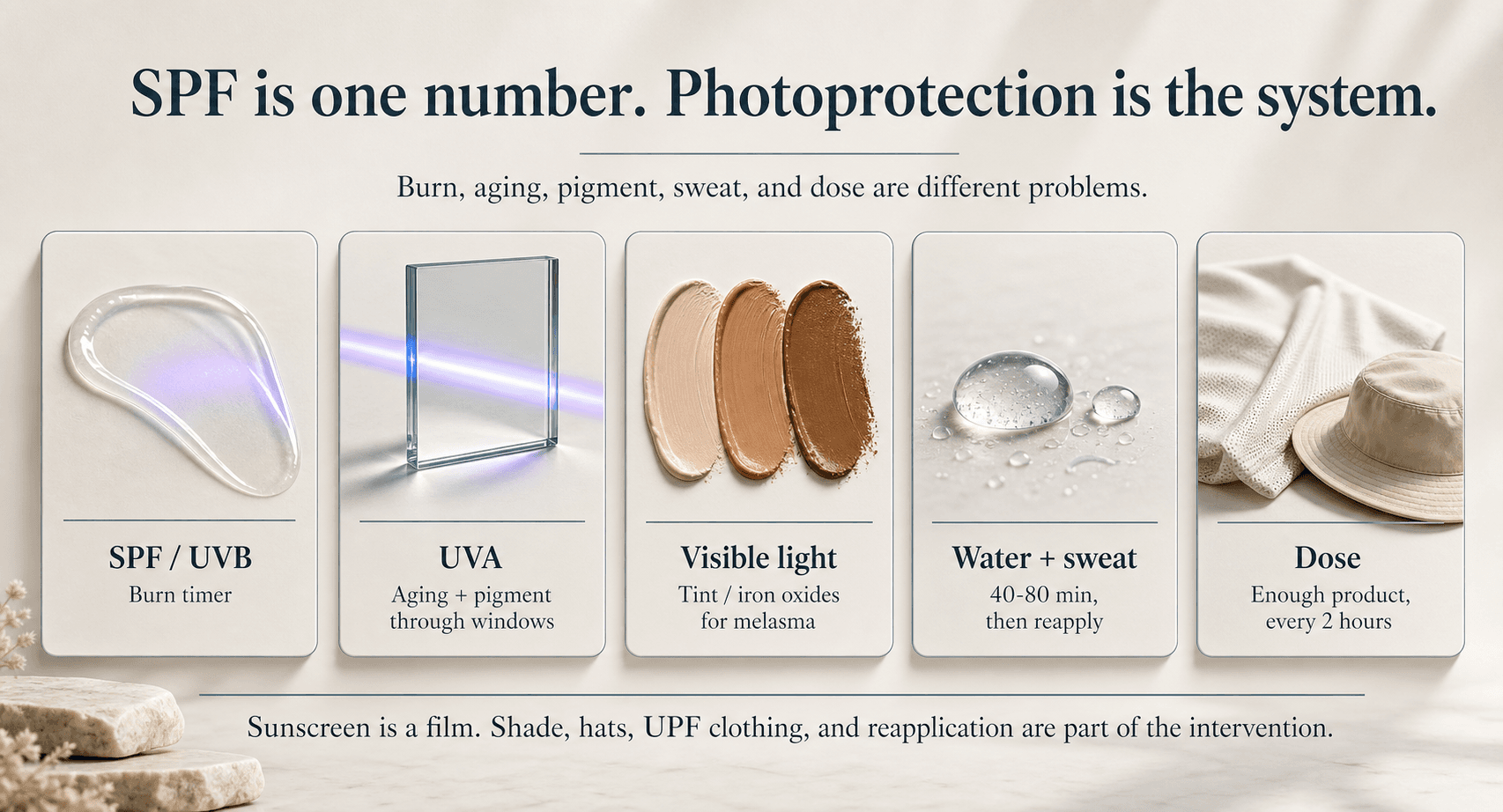
UVB
SPF is a sunburn score
Good for sunburn. Says little about aging, pigment, or daily use.
UVA
The aging wavelengths SPF ignores
UVA drives photoaging and pigment, and it passes through window glass.
Visible light
Tint blocks visible light
With melasma or PIH, clear sunscreen leaves visible light uncovered.
Water and sweat
Water resistance is timed
Swimming, sweat, and towels break the film down sooner.
Dose
Most people under-apply
The SPF on the label assumes far more product than most people apply.
Reapplication
Coverage fades through the day
A single morning layer will not cover a full day outdoors.
The core point is still simple: UV exposure is the established harm. Sunscreen used consistently and correctly has randomized human evidence for fewer skin cancers and less photoaging. These details are how you make that protection work in real life.

Real skin
The formula has to work on actual skin, not a lab label.
Pigment
Visible light is the gap clear SPF can miss.
Ingredients
Filter type is only one part of the decision.
Before you buy another bottle
Match sunscreen to the failure mode, not the prettiest SPF number.
If adherence is the problem, texture wins. If UVA or pigment is the problem, coverage and tint matter. If ingredient uncertainty bothers you, mineral lotion is the clean exit.
There is no such thing as sunblock
The FDA does not allow sunscreen labels to promise sunblock, waterproof, or sweatproof because no product blocks all sunlight or stays on indefinitely. Sunscreen is a thin protective film with failure modes: under-application, rubbing, sweating, swimming, poor UVA coverage, visible light, product aging, and sometimes ingredient uncertainty.
None of this makes sunscreen weak. But the question is not only “what SPF should I buy?” It is: which wavelengths are you trying to reduce, which skin outcome are you protecting, and will the product survive your actual day?
What sunscreen has actually been shown to do
Sunscreen is one of the few anti-aging consumer products with randomized human outcome evidence. In the Nambour trial, daily SPF 15+ use reduced squamous cell carcinoma tumor counts over 4.5 years compared with discretionary use. Long-term follow-up found fewer melanomas, especially invasive melanomas, although melanoma event counts were small, so I read that signal as suggestive rather than settled.
For visible skin aging, the same trial population showed 24% less measurable photoaging over 4.5 years in adults under 55. That is unusually good evidence for a drugstore product.
SPF is a burn timer, not a complete protection score
SPF mainly measures protection against erythema, or sunburn, which is driven largely by UVB. It does not directly grade UVA, visible light, water/sweat durability, real-world dose, or whether the product performs as labeled. The FDA’s broad-spectrum test uses a critical wavelength threshold, which is useful but still a pass/fail bar rather than a consumer-friendly UVA score.
This is why two SPF 50 products can behave very differently in real life. A 2022 in-vitro analysis of U.S. sunscreens found many products had much lower measured UVA protection than their SPF number would imply. I treat that study as a product-quality and labeling critique, not as proof every bottle is bad.
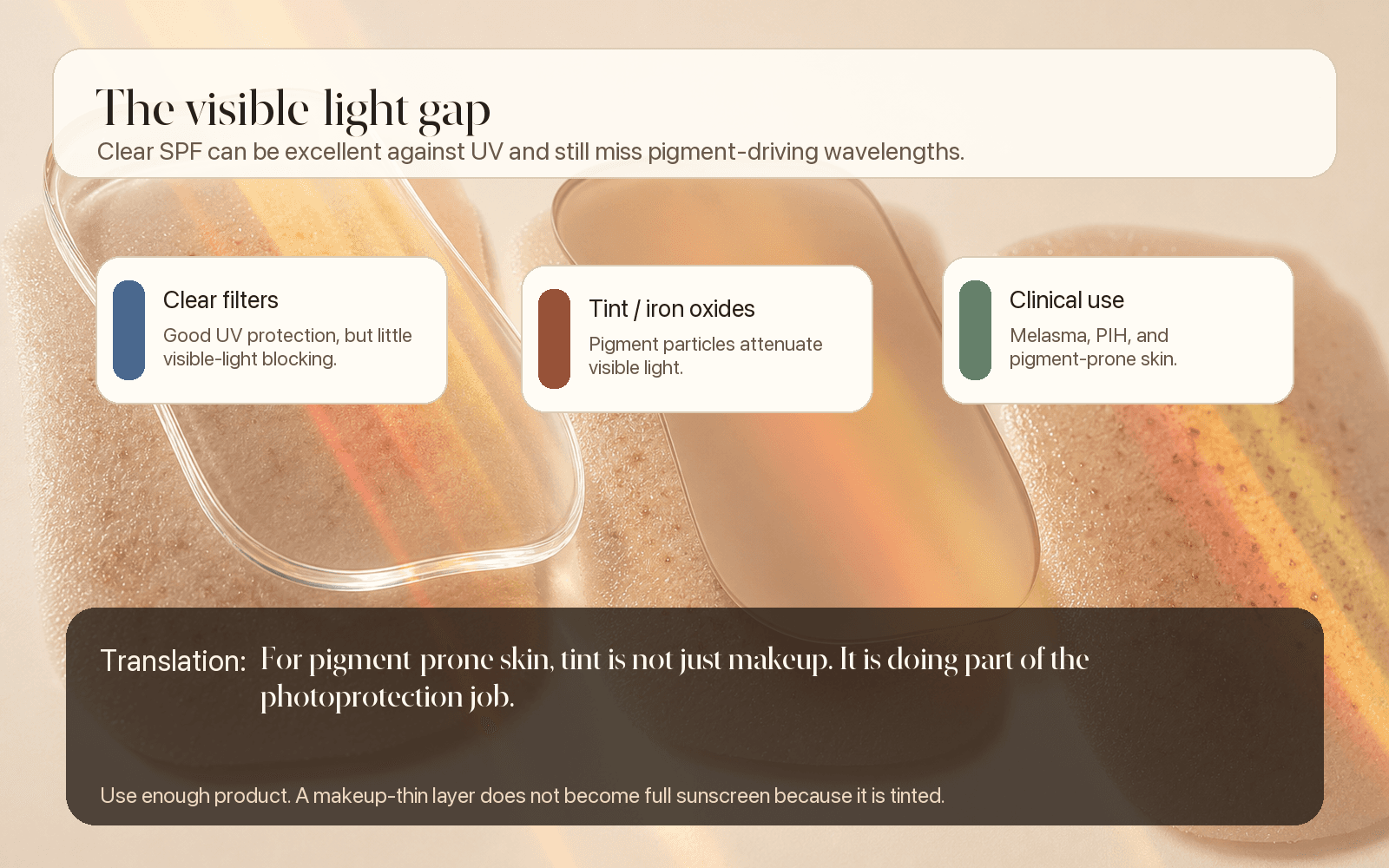
Visible light is the pigment gap most people miss
Ordinary visible light can worsen pigmentation, especially in darker phototypes and melasma-prone skin. Clear UV filters can be excellent against UV and still do little for visible light. That is where tint matters.
Tinted sunscreens with iron oxides physically reduce visible-light transmission. In melasma trials, UV plus visible-light protection outperformed UV-only sunscreen and helped reduce melasma relapse. Reviews of tinted sunscreens and visible-light photoprotection have continued to support this as a clinically useful lever for melasma, PIH, and pigment-prone skin.
If you are managing pigment, a clear SPF 50 may not be enough. You will likely need tint, an adequate amount, and a plan to reapply.
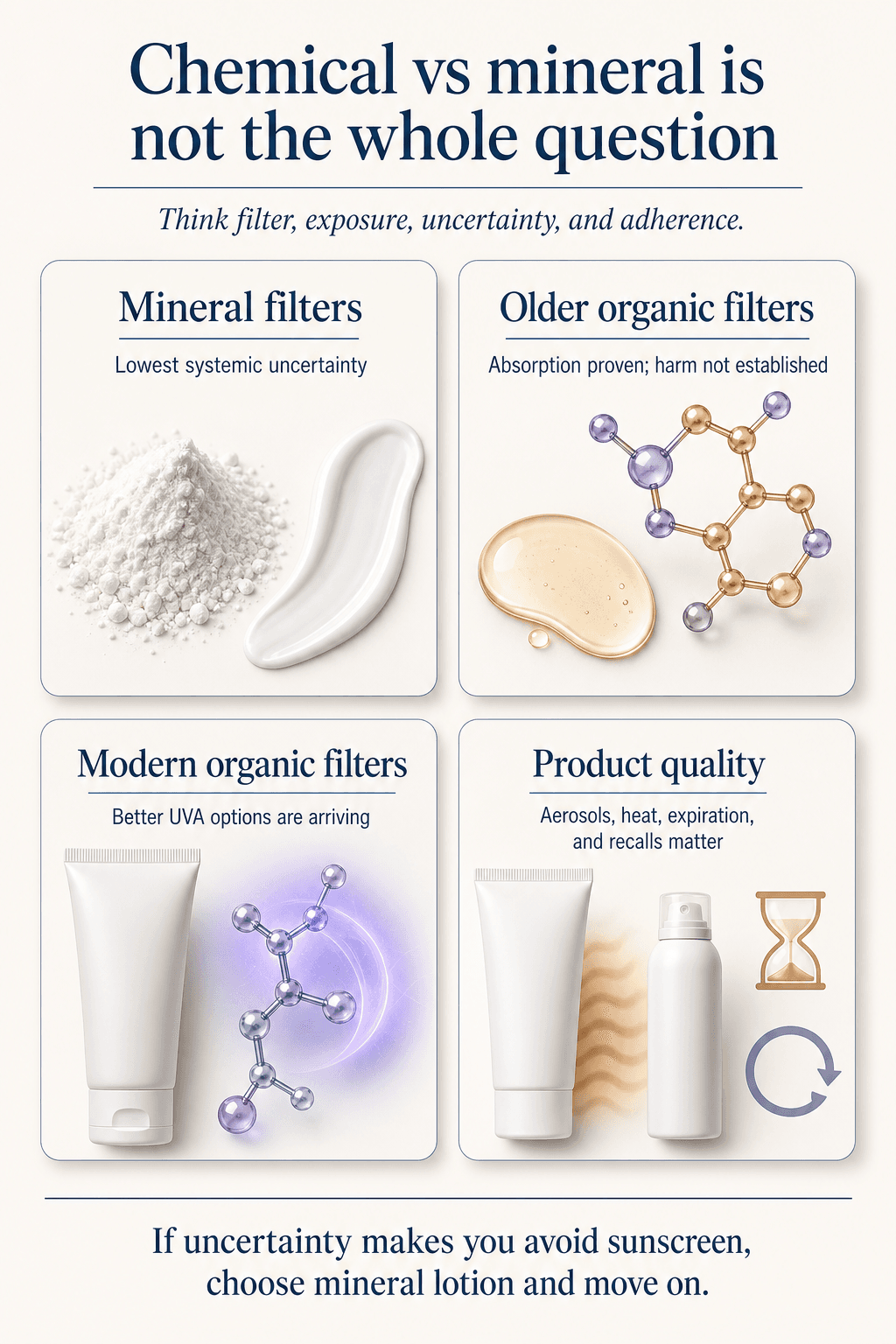
Mineral vs chemical sunscreen: what is proven, plausible, and not proven
Most people flatten this into either “chemical sunscreen is poison” or “there is nothing here.” The reality sits in between: some older organic filters are absorbed systemically; a few carry plausible endocrine or reproductive safety signals; and human harm at current sunscreen-use levels has not been established.
FDA maximal-use trials found avobenzone, oxybenzone, octocrylene, homosalate, octisalate, octinoxate, and ecamsule can reach blood levels above the FDA’s 0.5 ng/mL threshold. The 0.5 ng/mL line is a toxicology-data trigger, not a clinical harm threshold; the larger 2020 trial confirmed absorption across several common active ingredients.
For BP-3/oxybenzone specifically, a 2020 dermatology systematic review found insufficient evidence to establish causal human harm across major endocrine and reproductive endpoints. But a deeper 2023 HBM4EU review of BP-3/BP-1 argued that internal BP-3 concentrations after whole-body use may overlap with concentrations causing endocrine activity in vitro and adverse female reproductive effects in rodents, while human evidence includes mixed observational associations with menstrual hormones, fibroids, endometriosis, and other reproductive endpoints.
A 2023 ToxCast/Tox21 exposure-margin analysis found most common organic filters had low endocrine potency at measured human plasma concentrations; oxybenzone was the one filter where the exposure-to-bioactivity margin ran narrower. I single out BP-3/oxybenzone for the most caution rather than treating every chemical filter the same.
Homosalate is the second filter I treat cautiously: the EU Scientific Committee on Consumer Safety concluded it was not safe at 10% in its 2021 opinion and proposed much lower safe-use limits under that assessment. The same committee considered BP-3 not safe at 6% for body/spray sunscreens under its modeled conditions, while octocrylene was generally considered safe up to 10% for most uses but not at 10% in propellant spray under combined-use assumptions.
Octocrylene has a separate practical issue: contact and photocontact allergy, especially in adults with prior topical ketoprofen photoallergy, and possible product aging into benzophenone. The allergy pattern is described in photocontact allergy reviews; the degradation concern comes from work showing benzophenone accumulation from octocrylene in some commercial products over time.
Zinc oxide and titanium dioxide remain the lower-systemic-uncertainty topical default because intact-skin penetration is minimal and the FDA’s 2021 proposed order treated them as GRASE up to 25%. The caveat is form factor: sprays and powders raise inhalation concerns, and some mineral formulas underperform in independent testing. Mineral is lower uncertainty, not automatically better in every product.
Bemotrizinol is why the U.S. sunscreen conversation is changing
In June 2026, the FDA added bemotrizinol to the OTC sunscreen monograph, with the Federal Register final order allowing it up to 6%. Bemotrizinol is photostable, covers UVA and UVB well, and is barely absorbed. Europe and other markets have sold it for years as Tinosorb S; U.S. formulas should finally start to catch up.
Vitamin D is usually not a good reason to skip sunscreen
In controlled artificial-UV experiments, sunscreen can reduce vitamin D synthesis. In real life, field studies generally show little effect on vitamin D status, likely because humans do not apply sunscreen perfectly or everywhere. A 2019 review found real-world sunscreen use has little effect on vitamin D, and a high-UV Tenerife trial found optimal sunscreen use still allowed vitamin D synthesis while preventing sunburn.
If vitamin D is clinically relevant for you, measure it and supplement if needed. Do not use sunburn as dosing.
How to choose by use case
The best sunscreen is the one that fits the setting and actually gets used. Start with where you will wear it, then pick the product.
- Daily city / office: broad-spectrum SPF 30+ in a texture you will wear every morning. Tinted if pigment-prone.
- Driving / window UVA: prioritize stronger UVA coverage: zinc-rich mineral, EU/Asian high-UVA systems, or upcoming bemotrizinol formulas.
- Beach / sweat / workouts: water-resistant SPF 50+, full dose, applied before exposure, then reapplied every two hours and after swimming, sweating, or toweling.
- Melasma / PIH / deeper skin tones: tinted iron-oxide sunscreen, enough product, and reapplication. Do not apply it like thin foundation and expect full protection.
- Pregnancy / kids / risk-averse default: zinc or zinc/titanium lotion plus shade, hats, UPF clothing, and avoidance of aerosols around children.
- Reef or water destinations: UPF clothing first, mineral lotion on exposed skin, and follow local bans on oxybenzone or octinoxate.
Use-case selector
Use the table as a shortcut. There is rarely one universal sunscreen; there is the right one for the exposure and what you are trying to prevent.
Protocol
What to prioritize by setting
Daily errands / office
- Prioritize
- Broad-spectrum SPF 30+, texture you will actually wear, tint if pigment-prone
- Avoid relying on
- A perfect product you hate using
Driving / window exposure
- Prioritize
- Better UVA system, sunglasses, sleeves/gloves when practical
- Avoid relying on
- SPF number alone
Beach / sweat / workouts
- Prioritize
- SPF 50+, 80-minute water resistance, lotion/stick base, reapplication
- Avoid relying on
- Powder or mist SPF as the primary layer
Melasma / PIH
- Prioritize
- Tinted iron oxides plus enough product
- Avoid relying on
- Clear SPF as the only pigment strategy
Kids / pregnancy
- Prioritize
- Mineral lotion, shade, hats, UPF clothing; pediatrician guidance for infants under 6 months
- Avoid relying on
- Aerosols around children
Reef / water travel
- Prioritize
- UPF clothing, mineral lotion, local-rule compliance
- Avoid relying on
- Unregulated “reef safe” marketing
| Situation | Prioritize | Avoid relying on |
|---|---|---|
| Daily errands / office | Broad-spectrum SPF 30+, texture you will actually wear, tint if pigment-prone | A perfect product you hate using |
| Driving / window exposure | Better UVA system, sunglasses, sleeves/gloves when practical | SPF number alone |
| Beach / sweat / workouts | SPF 50+, 80-minute water resistance, lotion/stick base, reapplication | Powder or mist SPF as the primary layer |
| Melasma / PIH | Tinted iron oxides plus enough product | Clear SPF as the only pigment strategy |
| Kids / pregnancy | Mineral lotion, shade, hats, UPF clothing; pediatrician guidance for infants under 6 months | Aerosols around children |
| Reef / water travel | UPF clothing, mineral lotion, local-rule compliance | Unregulated “reef safe” marketing |
Ingredient safety quick map
This ranks uncertainty, not proven human harm. The harm from UV exposure is real and well established.
Protocol
Organic filter concerns in context
BP-3 / oxybenzone
- What is most plausible
- Strongest endocrine/reproductive plausibility signal among older U.S. filters; mixed observational human data
- Practical read
- Avoid if easy, especially for pregnancy, children, or high-frequency large-area use
Homosalate
- What is most plausible
- Regulatory margin-of-safety and endocrine-uncertainty concern at higher concentrations
- Practical read
- Reasonable to avoid in risk-averse scenarios
Octocrylene
- What is most plausible
- Photoallergy/contact allergy and benzophenone-degradant concerns more than settled endocrine harm
- Practical read
- Do not use expired/heat-stored products; avoid if photoallergic
Avobenzone / octisalate / octinoxate
- What is most plausible
- Lower current endocrine concern by ToxCast/human-weight-of-evidence, but still in FDA data-gap category
- Practical read
- Can be reasonable if product performance/adherence is better
Zinc oxide / titanium dioxide
- What is most plausible
- Low topical systemic absorption; inhalation is the form-factor caveat
- Practical read
- Best low-uncertainty default as lotion/stick
| Filter / issue | What is most plausible | Practical read |
|---|---|---|
| BP-3 / oxybenzone | Strongest endocrine/reproductive plausibility signal among older U.S. filters; mixed observational human data | Avoid if easy, especially for pregnancy, children, or high-frequency large-area use |
| Homosalate | Regulatory margin-of-safety and endocrine-uncertainty concern at higher concentrations | Reasonable to avoid in risk-averse scenarios |
| Octocrylene | Photoallergy/contact allergy and benzophenone-degradant concerns more than settled endocrine harm | Do not use expired/heat-stored products; avoid if photoallergic |
| Avobenzone / octisalate / octinoxate | Lower current endocrine concern by ToxCast/human-weight-of-evidence, but still in FDA data-gap category | Can be reasonable if product performance/adherence is better |
| Zinc oxide / titanium dioxide | Low topical systemic absorption; inhalation is the form-factor caveat | Best low-uncertainty default as lotion/stick |
Application rules that matter more than product ideology
Apply roughly one ounce, a shot-glass amount, for an adult body when in a swimsuit-level exposure setting.
Apply before exposure and reapply at least every two hours outdoors, plus after swimming, sweating, or toweling.
Do not forget ears, lips, back of neck, hands, tops of feet, hairline, scalp part, and the area around sunglasses or hat edges.
Use sprays only if you spray until skin glistens and rub it in; avoid inhaling them and avoid open flame.
Do not treat powder sunscreen as beach sunscreen. It is a touch-up tool, not a primary protective film.
Clinical lens
How I’d decide
Use this section as a second pass after the main answer, not as homework before you know what the page is saying.
Who it’s for
Adults choosing sunscreen for daily prevention, photoaging, pigment, driving/window exposure, outdoor activity, sensitive skin, pregnancy/family use, or reef/water trips.
Who should skip it
Use this as education, not personal medical care, if you have melanoma history, immunosuppression, lupus/porphyria/photosensitivity disorders, severe photoallergy, extensive actinic keratoses, suspicious lesions, or medication-driven photosensitivity.
Measure before / after
Look at the actual use case: daily adherence, UVA/PA or zinc-rich coverage, tint/iron oxides for pigment, water resistance for sweat/swim, expiration/storage, and whether you can realistically reapply.
What I’d do first
Choose for the problem you actually have. If you will not reapply, pick a texture you will wear. If photoaging worries you, prioritize UVA coverage. For pigment, use a tinted iron-oxide formula. If older organic filters make you uneasy, use a zinc or titanium lotion and move on.
What would change my mind
Better long-term human endocrine/reproductive outcome data for older organic filters, broader independent testing of bemotrizinol formulas, stronger U.S. UVA labeling, and more product-quality surveillance would change the practical ranking.
Frequently Asked Questions
What does SPF actually mean?
SPF estimates how much longer protected skin takes to develop UVB-driven redness under test conditions. It is not a complete score for UVA, visible light, water/sweat, dose, or product quality.
Is SPF 50 much better than SPF 30?
SPF 50 blocks a little more UVB under test conditions, but real-world dose and reapplication often matter more. For high sun, I prefer SPF 50+ because humans under-apply.
Do I need tinted sunscreen?
Not always. Tint matters most when visible light is part of the problem: melasma, post-inflammatory hyperpigmentation, and pigment-prone skin. For skin cancer prevention alone, a clear broad-spectrum sunscreen can be enough if you use it properly.
What should I look for if I want better UVA protection?
In the U.S., broad spectrum is the minimum, but it is not a precise UVA score. For stronger UVA coverage, look for PA++++ or the EU UVA seal on international products, zinc-rich mineral formulas, or newer high-UVA filters such as bemotrizinol as U.S. formulas become available.
How do I choose sunscreen for my face?
Start with the texture you will actually wear daily: lotion, cream, gel, no eye sting, non-comedogenic if acne-prone, tinted if pigment-prone, and broad-spectrum SPF 30+. For outdoor days, use SPF 50+ and reapply; makeup SPF alone is not enough.
Is mineral sunscreen safer than chemical sunscreen?
On systemic absorption, zinc oxide and titanium dioxide carry less uncertainty. But a mineral sunscreen that performs poorly is not automatically better than a strong organic or hybrid formula that someone actually uses well.
Are chemical sunscreens endocrine disruptors?
Some older organic filters are systemically absorbed and have plausible endocrine or reproductive signals, especially BP-3/oxybenzone and homosalate. Human causal harm at current sunscreen-use levels has not been established.
Is spray sunscreen okay?
It can be used carefully as a rubbed-in layer or top-up, but I would not make aerosols the default for children or high-exposure days. Coverage is uneven, inhalation matters, and some aerosol categories have had contamination recalls.
Does sunscreen block vitamin D?
In artificial-UV experiments it can reduce synthesis, but real-world studies generally do not show meaningful vitamin D compromise from normal sunscreen use. Test and supplement if needed rather than using sunburn as a dose.
What is bemotrizinol?
Bemotrizinol is a modern, photostable UVA/UVB filter the FDA added to the U.S. OTC sunscreen monograph in 2026. It has been available in other markets as Tinosorb S and has low skin absorption.
References & citations
- 1.FDA 2011 sunscreen labeling rule: sunblock/waterproof/sweatproof claims
- 2.Green et al. Daily sunscreen and SCC/BCC prevention, Lancet 1999
- 3.Green et al. Reduced melanoma after regular sunscreen use, J Clin Oncol 2011
- 4.Hughes et al. Sunscreen and prevention of skin aging, Ann Intern Med 2013
- 5.Andrews et al. U.S. sunscreen label/in-vitro SPF and UVA testing critique, 2022
- 6.Lyons et al. Photoprotection beyond ultraviolet radiation: tinted sunscreens, JAAD 2021
- 7.Castanedo-Cazares et al. Near-visible light and UV photoprotection in melasma, 2014
- 8.Boukari et al. Preventing melasma relapse with UV and visible-light protection, 2015
- 9.Matta et al. Sunscreen active ingredient absorption under maximal use, JAMA 2019
- 10.Matta et al. Six sunscreen active ingredients systemic absorption, JAMA 2020
- 11.Suh et al. Oxybenzone/octinoxate human health systematic review, 2020
- 12.Mustieles et al. BP-3 toxicology and human biomonitoring review/meta-analysis, 2023
- 13.Onyango et al. ToxCast/Tox21 endocrine activity vs human plasma levels, 2023
- 14.SCCS Opinion on Benzophenone-3, 2021
- 15.SCCS Opinion on Homosalate, 2021
- 16.SCCS Opinion on Octocrylene, 2021
- 17.de Groot and Roberts. Contact and photocontact allergy to octocrylene, 2014
- 18.Downs et al. Benzophenone accumulation from octocrylene degradation, 2021
- 19.FDA adds bemotrizinol to OTC sunscreen monograph, 2026
- 20.Federal Register final order adding bemotrizinol up to 6%, 2026
- 21.FDA 2021 proposed administrative order on sunscreen monograph/GRASE filters
- 22.Neale et al. Sunscreen and vitamin D review, 2019
- 23.Young et al. Optimal sunscreen use allows vitamin D synthesis without sunburn, 2019
- 24.AAD: how to select and apply sunscreen
- 25.FDA FAQ on benzene contamination in drugs
Photoprotection next step
The low-uncertainty default is boring, and that is the point.
If you are pregnant, buying for kids, covering large areas daily, or simply risk-averse, choose zinc or titanium lotion plus shade, hats, UPF clothing, and reapplication.