Sleep medications and supplements: what helps, what is risky, and why sedation is not sleep
Sedation is not the same as restorative sleep. For chronic insomnia, CBT-I has the strongest durable evidence; medications and supplements work best when matched to the sleep pattern, mechanism, sleep architecture, next-day function, and safety context.
First-line
For chronic insomnia, CBT-I is the foundation; sleep hygiene is useful background, not the treatment itself.
Match the pattern
Sleep pressure, circadian timing, hyperarousal, and continuity/breathing problems need different tools.
Safety first
OTC antihistamines, sedative stacking, alcohol, older age, fall risk, and breathing disorders deserve extra caution.
Short answer
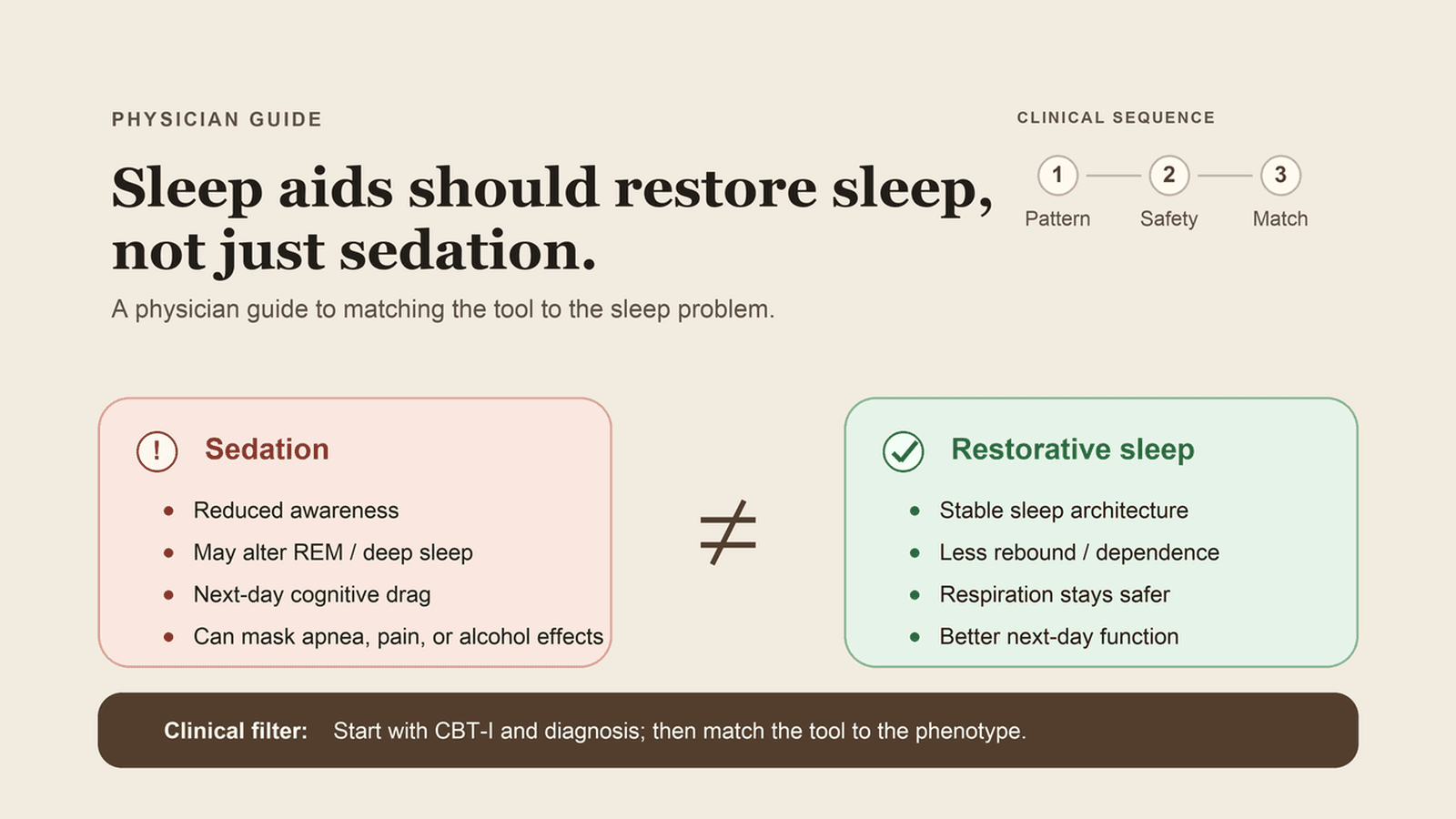
Sedation is not sleep.
That is the most important idea in this guide. A medication can make you less aware, shorten the time it takes to drift off, or make the night feel easier. But physiologic sleep is not just unconsciousness. [1] It is a structured, cycling state with timing, depth, continuity, breathing, temperature, hormones, memory processing, and recovery built into it.
If you only remember five things:
- For chronic insomnia, CBT-I comes first because the evidence is unusually practical: randomized trials and meta-analyses show improvements in insomnia severity, sleep efficiency, sleep latency, and wake after sleep onset, with benefits that can persist after treatment. Sleep hygiene is background; CBT-I is the structured intervention. Guidelines mirror that evidence; they are not the reason for the recommendation. [3,4,45-47]
- The right sleep aid depends on the sleep pattern. Trouble falling asleep, repeated awakenings, early-morning waking, jet lag, and tired-but-wired hyperarousal are not the same problem.
- OTC does not mean benign. Diphenhydramine and doxylamine are especially poor repeated-use choices for older adults, fall-prone patients, and anyone with cognitive vulnerability. [2,5]
- DORAs are interesting because they turn down wake drive. That is different from simply pushing GABAergic sedation, but they are still prescription hypnotics with next-day, mood, respiratory, and interaction cautions. The frontier data are strongest for sleep continuity and architecture signals, not long-term brain protection. [2,8-13,38-44]
- Most supplements have modest, conditional, or preliminary evidence. A few may be reasonable in the right person; none should replace evaluation for sleep apnea, restless legs, pain, alcohol rebound, hot flashes, mood symptoms, or medication effects.
The better question is not, "What can knock me out?"
It is: "Which sleep system is failing, and what is the safest way to restore it?"
This is an educational guide, not individualized medical advice. If you have persistent insomnia, complex medical conditions, pregnancy or lactation, breathing problems, fall risk, cognitive symptoms, or you take other medications, talk with your clinician before using sleep medications or supplements.
Last reviewed: June 3, 2026. References and PubMed-backed citations were checked against the linked research note and NCBI/PubMed metadata on June 3, 2026.
The simplest decoder: restorative sleep, sedation, and unconsciousness are different states
People often use these words interchangeably. They should not.
Restorative sleep
Restorative sleep is an active physiologic state. The brain cycles through NREM and REM sleep. Heart rate and blood pressure fall. Growth hormone pulses during deep sleep. Memory is consolidated. Emotional processing shifts. Metabolic and immune signals change. Breathing stays stable. The nervous system gets a real chance to come down.
Restorative sleep has architecture. It has rhythm. It has continuity.
Sedation
Sedation means reduced alertness. It can feel like sleep from the inside because you are less aware. But sedatives do not automatically reproduce normal sleep architecture. Some suppress REM. Some alter deep sleep. Some fragment the second half of the night. Some leave you impaired the next morning. Some make you less likely to notice that breathing, alcohol rebound, reflux, pain, restless legs, or hot flashes are still breaking your sleep.
A stronger sedative is not always a smarter sleep plan.
Unconsciousness
Unconsciousness is even less specific. Anesthesia, intoxication, severe illness, and head injury can all reduce consciousness. Nobody would call those healthy sleep.
This is why "I was out cold" is not the same as "I recovered."
Quick evidence key
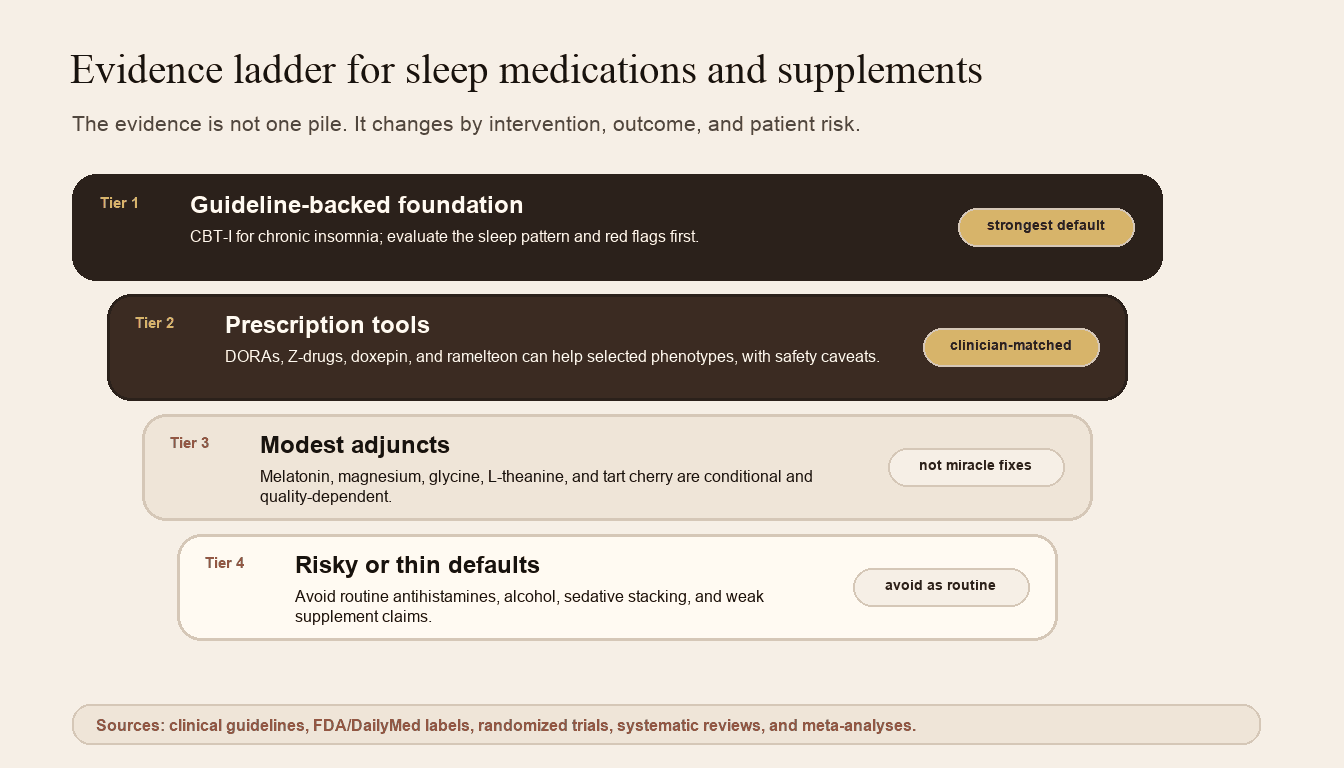
The evidence differs by intervention, outcome, and patient risk.
This guide uses a practical evidence ladder:
- Strong / first-line: consistent trial and meta-analysis evidence with durable benefit and a favorable safety profile, especially CBT-I for chronic insomnia.
- Reasonable when matched to the pattern: FDA-approved insomnia medications with RCT data, used for the right phenotype and risk profile.
- Modest or conditional: supplements or medications with small effect sizes, limited populations, or context-specific use.
- Caution / avoid as routine sleep aids: choices where repeated use often creates more risk than benefit, especially benzodiazepines, Z-drugs in older adults, and anticholinergic OTC antihistamines.
The four sleep systems I would check before choosing a sleep aid
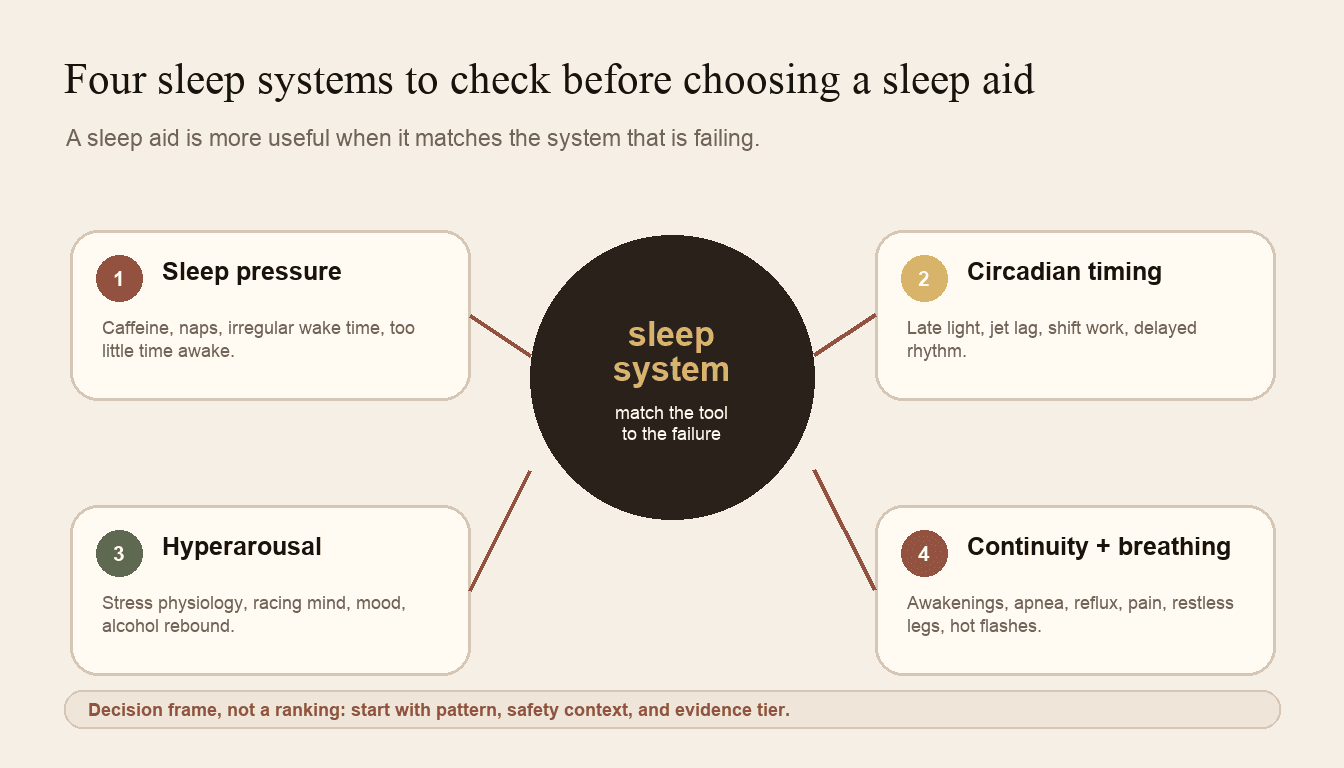
Start by identifying which sleep system is failing before choosing a medication or supplement.
Insomnia is not one problem. It is a symptom pattern. The right tool depends on the broken system.
Clinical decoder
Four sleep systems decoder
Clinical rule
Pattern first, tool second. A sleep aid is safer and more useful when it matches the sleep system that is actually failing.
Sleep pressure
Tired, but not sleepy enough.
Check first
Naps, caffeine timing, irregular wake time, low activity, too much awake time in bed.
Usually helps
CBT-I, stable wake time, stimulus control, and rebuilding sleep drive.
Caution
Hypnotics can hide a weak sleep-pressure problem.
Circadian timing
Sleepy at the wrong time.
Check first
Light exposure, wake time, travel, shift work, delayed schedule, and meal/activity timing.
Usually helps
Light timing, wake-time anchoring, and melatonin or ramelteon when appropriate.
Caution
Melatonin is a clock signal, not a knockout drug.
Hyperarousal
Tired but wired.
Check first
Stress, pain, alcohol rebound, stimulants, thyroid excess, PTSD/panic, and high evening cognitive load.
Usually helps
CBT-I, stimulus control, relaxation or breathing work, medication review, and treating the driver.
Caution
Stronger sedation can miss the real problem.
Sleep architecture + continuity
Sleep happens, but does not restore.
Check first
Apnea, restless legs, reflux, nocturia, hot flashes, alcohol, pain, and medications that fragment sleep.
Usually helps
Diagnose and treat the fragmentation source before escalating sleep aids.
Caution
Do not sedate over untreated apnea or breathing risk.
1. Sleep pressure
Sleep pressure builds the longer you are awake. Adenosine is one of the key signals here. Caffeine blocks adenosine signaling, which is why coffee can make a tired brain feel falsely alert.
Sleep pressure gets weaker when:
- you nap too long or too late
- your wake time shifts around
- caffeine runs too late into the day
- activity is low
- you spend too much time in bed awake
- alcohol fragments the night, especially the second half
If sleep pressure is the problem, a hypnotic may hide the issue without fixing it. A CBT-I plan often works here because it rebuilds the relationship between time in bed, sleep drive, and actual sleep.
2. Circadian timing
Your circadian system tells your brain when sleep is biologically available. It is shaped by light, wake time, meals, activity, temperature, travel, and shift work.
Circadian timing is often the issue when someone says:
- "I am not sleepy until 1 or 2am."
- "I sleep fine if I can sleep late."
- "Jet lag destroys me."
- "My schedule changes every few days."
- "Melatonin worked once, then stopped."
Melatonin and ramelteon belong in this category. They are better understood as timing signals than as knockout drugs. Timing and dose matter more than force.
Melatonin is a clock signal, not a hammer.
3. Hyperarousal
Hyperarousal is the tired-but-wired pattern. The body is exhausted, but the nervous system is still scanning, solving, rehearsing, worrying, or guarding.
Common drivers include:
- stress and anxiety
- pain
- conditioned wakefulness in bed
- alcohol rebound
- overtraining
- stimulant medications
- thyroid excess
- PTSD or panic symptoms
- high evening cognitive load
This is where CBT-I, stimulus control, relaxation, breathing, stress treatment, pain care, and medication review often matter more than adding a stronger sedative. In some patients, a DORA medication may make physiologic sense because it lowers wake signaling through the orexin system rather than simply pushing GABAergic sedation.
4. Sleep architecture and continuity
Sleep is not one flat state. It cycles through light sleep, deep NREM sleep, and REM sleep. The pattern matters.
A person can spend eight hours in bed and still get poor sleep if the night is fragmented by:
- obstructive sleep apnea
- COPD, hypoventilation, or other breathing problems
- restless legs or periodic limb movements
- nocturia
- reflux
- pain
- hot flashes or night sweats
- alcohol
- depression with early-morning awakening
- medications that disturb sleep architecture
If a medication "works" by making you less aware while apnea, limb movements, alcohol rebound, or pain continue, the problem is not solved. It is muffled.
Before you choose a sleep aid, rule out the “not just insomnia” problems
Some sleep problems should not be treated by simply adding sedation.
Get evaluated, or at least pause before self-treating, if the pattern includes:
- loud snoring, witnessed apneas, choking or gasping, morning headaches, resistant hypertension, or major daytime sleepiness
- restless legs, crawling sensations, kicking, or repeated limb movements
- severe depression, suicidality, mania or hypomania, PTSD nightmares, panic attacks, or a major recent mood change
- chronic pain, reflux, nocturia, hot flashes, thyroid symptoms, pregnancy/postpartum symptoms, or new neurologic symptoms
- alcohol rebound waking, opioid use, COPD, known sleep apnea, hypoventilation, neuromuscular disease, or other breathing-risk states
- older age, frailty, cognitive impairment, delirium history, fall risk, or early-morning driving/safety-sensitive work
If a medication “works” by making you less aware while apnea, alcohol rebound, limb movements, or pain continue, the sleep problem has not been solved. It has been muffled.
Why CBT-I comes before a sleep aid
Sleep hygiene is background. CBT-I is treatment.
Sleep hygiene says: keep the room cool, avoid screens late, limit caffeine, get morning light. Useful, but usually not enough for chronic insomnia.
CBT-I is more specific. It usually includes:
- Stimulus control: retraining the bed as a cue for sleep, not wakeful problem-solving.
- Sleep restriction or sleep compression: reducing excess time in bed to rebuild sleep drive and sleep efficiency.
- Cognitive work: changing the fear loop around sleep without pretending insomnia is "all in your head."
- Relaxation and arousal reduction: lowering sympathetic activation.
- Circadian structure: consistent wake time, light timing, and behavioral anchors.
CBT-I has a stronger claim than sleep hygiene because it retrains the sleep system: stimulus control weakens bed-awake conditioning, sleep restriction or compression consolidates sleep drive, cognitive work reduces threat monitoring, relaxation lowers arousal, and circadian anchors stabilize timing. In RCT-heavy evidence syntheses, CBT-I improves insomnia severity, sleep efficiency, sleep-onset latency, and wake after sleep onset; guideline statements sit downstream of that trial evidence. [45-47]
That does not mean medication is never appropriate. It means medication should not be the only plan when the underlying sleep system is trainable.
A practical way to frame it:
- If insomnia is acute, short-term medication may sometimes be reasonable.
- If insomnia is chronic, CBT-I should be part of the plan.
- If insomnia is persistent or worsening, evaluate for medical, psychiatric, respiratory, hormonal, pain, medication, and substance-related contributors.
One caveat: sleep restriction can temporarily increase daytime sleepiness. It needs extra care in people with bipolar disorder, seizure risk, high-risk driving, pregnancy, frailty, unsafe daytime sleepiness, or safety-sensitive work.
Medication decoder
This section is not a ranking of "best sleep drugs." It is a physiology and safety decoder.
Medication map
Sleep medication mechanism map
How to read this section
Medication classes differ by the sleep system they target. The useful question is not ‘what is strongest?’ It is ‘what problem is this treating, and what risk is it adding?’
DORAs
OrexinCommon names
Best fit
Sleep-maintenance insomnia, frequent awakenings, hyperarousal, and difficulty staying asleep.
Main caution
Can still cause next-day impairment, abnormal dreams, sleep paralysis, complex sleep behaviors, and additive sedation. Not dementia prevention.
Z-drugs
GABA-ACommon names
Best fit
Short-term sleep-onset or maintenance help in selected adults when safer contributors have been addressed.
Main caution
FDA boxed warning for complex sleep behaviors; also consider falls, fractures, rebound insomnia, tolerance, and driving risk.
Benzodiazepines
GABACommon names
Best fit
Rarely a good chronic-insomnia choice; sometimes used short-term for specific anxiety, withdrawal, or procedural contexts.
Main caution
Dependence, withdrawal, cognitive impairment, falls, crashes, respiratory risk, and worse sleep architecture.
Low-dose doxepin
HistamineCommon names
Best fit
Sleep-maintenance insomnia and early awakenings when the issue is staying asleep.
Main caution
Dose matters. Higher antidepressant-range dosing is a different risk profile, especially for anticholinergic burden.
Ramelteon
Clock signalCommon names
Best fit
Sleep-onset insomnia or circadian-timing problems where signaling biological night is the point.
Main caution
Not a knockout drug. Timing and patient phenotype matter more than force.
OTC antihistamines
AnticholinergicCommon names
Best fit
Not a routine chronic sleep strategy; occasional use still deserves caution.
Main caution
Confusion, delirium, urinary retention, constipation, falls, next-day impairment, and fast tolerance, especially in older adults.
Examples are common U.S. names/formulations, not endorsements; names vary by product and country, and some uses may be off-label.
How I read the frontier evidence
From first principles, a sleep-medication claim has to answer different questions: does it shorten sleep latency, reduce wake time after sleep onset, increase total sleep time, preserve sleep architecture, improve next-day function, or change a biomarker? Those endpoints are related, but they are not interchangeable.
That matters most for trazodone and DORAs. Trazodone may improve perceived sleep quality or awakenings and may shift PSG architecture toward less N1 and more N3 in some studies, but that does not prove more restorative sleep or long-term brain benefit. DORAs have a cleaner mechanistic story for hyperarousal because they reduce orexin wake signaling; newer architecture analyses suggest less wake persistence with relatively preserved N2, N3, and REM spectral features. That still is not dementia-prevention evidence. [13,34-44]
The frontier evidence I would watch is sleep-stage physiology, EEG signatures of hyperarousal, next-day function, respiratory safety in real-world patients, and biomarker work such as amyloid-beta and tau. The public standard should stay higher than “this changes a lab marker” or “this made someone sleepy.”
DORAs: suvorexant, lemborexant, daridorexant
DORAs are dual orexin receptor antagonists. Orexin helps stabilize wakefulness. In insomnia with hyperarousal or repeated awakenings, the first-principles appeal is that a DORA reduces wake drive instead of broadly pushing GABAergic sedation.
That is a meaningful mechanistic difference, not proof that DORAs are best for everyone. The clinical question is endpoint-specific: sleep onset, wake after sleep onset, total sleep time, sleep architecture, next-day function, and safety should be judged separately.
Best fit: sleep-maintenance insomnia, frequent awakenings, hyperarousal, and difficulty staying asleep. Some DORAs can also help sleep onset, depending on the agent, dose, and patient pattern.
Evidence: suvorexant, lemborexant, and daridorexant have randomized trial data showing improvements in sleep-maintenance and/or sleep-onset measures versus placebo. Lemborexant has older-adult data against zolpidem ER, and daridorexant 50 mg improved selected daytime-functioning measures in phase 3 trials. Recent network meta-analyses support class efficacy, but they do not make the three agents interchangeable. [11,12,38,42,44]
Architecture and frontier physiology: suvorexant PSG analyses suggest overall sleep architecture is largely preserved, with increased minutes in all stages and small REM shifts. Lemborexant architecture analyses in older adults and daridorexant EEG analyses point toward better continuity and less wake persistence rather than global stage suppression. In a post hoc phase 3 analysis, daridorexant 50 mg reduced wake-to-wake transition probability and wake/N1 beta power without materially altering N2, N3, REM spectral bands, or spindle activity. [39-41]
Safety caveats: DORAs can still cause somnolence, next-day impairment, abnormal dreams, sleep paralysis, hallucination-like experiences around sleep, cataplexy-like symptoms, complex sleep behaviors, mood worsening or suicidal ideation, and additive sedation with alcohol or other CNS depressants. A 2024 safety meta-analysis found higher treatment-emergent adverse events and excessive daytime sleepiness with DORAs versus placebo. Narcolepsy is a contraindication, and breathing risk needs caution in people with obstructive sleep apnea, COPD, hypoventilation, obesity hypoventilation, neuromuscular disease, opioid use, or other compromised respiratory function. [8-10,43]
Longevity and Alzheimer caveat: suvorexant acutely lowered CSF amyloid-beta and tau phosphorylation in a small study of cognitively unimpaired adults. That is a mechanistic biomarker clue, not proof of cognitive benefit, Alzheimer prevention, or healthspan extension. Do not market DORAs as dementia-prevention drugs. [13]
Plain English: DORAs are a more physiology-aware class for some patients, especially wake-drive and maintenance problems, but they are still hypnotics—not a free pass.
Z-drugs: zolpidem, zaleplon, eszopiclone
Z-drugs are sedative-hypnotics that act through GABA-A receptor modulation. They can reduce sleep latency and sometimes help maintenance depending on the drug and formulation.
Best fit: selected short-term use when the benefit is clear, the sleep opportunity is adequate, and safety risks are low.
Main concern: they can make sleep feel solved while shifting risk into the next morning.
The FDA added a boxed warning for complex sleep behaviors with zolpidem, zaleplon, and eszopiclone. [6,7] These include sleepwalking, sleep driving, preparing or eating food, making calls, and other activities while not fully awake. Serious injuries and deaths have been reported.
Other risks include next-day impairment, driving risk, falls, fractures, rebound insomnia, tolerance, misuse, cognitive effects, and dangerous combinations with alcohol, opioids, benzodiazepines, gabapentinoids, antipsychotics, muscle relaxants, sedating antihistamines, and other CNS depressants.
For older adults, the caution is not simply that Beers says so. Z-drugs produce only modest average sleep benefits, while FDA warnings and observational safety data point to complex sleep behaviors, serious injury, falls/fractures, cognitive effects, and driving risk. The 2023 Beers Criteria are a concise safety summary of that risk-benefit asymmetry. [5-7,48]
Plain English: useful in narrow situations, but not a casual long-term sleep plan.
Benzodiazepines
Benzodiazepines are the clearest example of the gap between sedation and sleep. They can reduce anxiety and cause sedation, but that does not mean they restore physiologic sleep.
Best fit: not a preferred chronic insomnia strategy. They may be used in narrow, short-term, supervised contexts, often when there is another indication.
Risks: dependence, tolerance, withdrawal, rebound insomnia, cognitive impairment, delirium, falls, fractures, motor vehicle crashes, and respiratory depression, especially when combined with other depressants.
For older adults, benzodiazepines are generally a poor sleep choice because the pharmacology and outcome risks are predictable: tolerance, dependence, withdrawal, delirium or cognitive impairment, falls, fractures, crashes, and respiratory depression with other depressants. Beers is useful as a safety flag, but the reason is the risk biology and observed harms. [5,48]
Plain English: benzodiazepines may make you unconscious, but unconscious is not the same as restored.
Low-dose doxepin
Doxepin is confusing because dose changes the clinical story. At antidepressant doses, it is a tricyclic antidepressant with more anticholinergic and cardiac considerations. At very low insomnia doses, usually 3 to 6 mg, it mainly works through histamine H1 antagonism.
Best fit: sleep-maintenance insomnia, repeated awakenings, or early awakenings with trouble returning to sleep.
Not the best fit: pure sleep-onset insomnia.
Low-dose doxepin earns a place as a maintenance tool because placebo-controlled trials show sleep-maintenance benefits, not because it broadly sedates. The signal is small-to-moderate, longer-term data are limited, and some of the evidence base has industry involvement. [14]
Safety caveats: somnolence, headache, next-day effects in susceptible people, and caution with other sedatives. Doxepin doses above 6 mg/day are a Beers Criteria concern because anticholinergic effects become more relevant.
Plain English: low-dose doxepin is a maintenance tool, not a knockout pill.
Ramelteon and the melatonin pathway
Ramelteon is a melatonin receptor agonist. It is not a broad sedative. It signals biological night.
Best fit: sleep-onset insomnia, delayed sleep timing, circadian rhythm problems, and people where abuse or dependence risk is a major concern.
Ramelteon has meta-analysis evidence for modest sleep-onset effects, which fits its melatonin-receptor and circadian mechanism. That is not a failure. It means ramelteon should be used for the right problem: timing, not brute-force sedation. [16]
Safety caveats: hepatic impairment, drug interactions, pregnancy and lactation context, and next-day function still matter.
Plain English: ramelteon is a clock tool.
Trazodone and other off-label sedating antidepressants
Trazodone is one of the most common off-label sleep prescriptions. Common does not mean best supported, and “it makes me sleepy” is not the same claim as “it improves insomnia safely.”
Mechanistically, trazodone is not a targeted insomnia-circuit drug. At lower sleep doses, its sedating effects likely come through histamine H1, serotonin 5-HT2A, and alpha-1 adrenergic effects. That can reduce arousal, but it also explains common tradeoffs such as dizziness, orthostasis, and next-day impairment. What keeps it from being a reflex chronic-insomnia default is not committee taste; it is the benefit/risk evidence: trials and meta-analyses show mixed-to-modest insomnia benefit, selected PSG architecture signals, and real adverse-event or next-day impairment tradeoffs. [34-37]
Evidence in primary insomnia: a small randomized PSG study of trazodone 50 mg for 7 nights found fewer awakenings, less N1 light sleep, and more slow-wave sleep by day 7. The same study found small but significant next-day impairments in short-term memory, verbal learning, equilibrium, and muscle endurance. [34]
Systematic reviews are mixed-to-modest rather than cleanly negative. A 2018 meta-analysis found improved perceived sleep quality and fewer awakenings, but no significant improvement in sleep latency, total sleep time, sleep efficiency, or WASO. A 2024 meta-analysis across broader sleep-problem contexts found improvements in sleep quality, awakenings, WASO, and objective PSG total sleep time, while subjective total sleep time was not clearly improved and adverse effects or dropouts increased. [35,36]
Architecture: trazodone may reduce N1/awakenings and increase N3 or slow-wave sleep in PSG studies. That is physiologically interesting, but it should not be translated into “restorative sleep,” cognition protection, glymphatic clearance, dementia prevention, or long-term health benefit. [34,37]
Potential role: selected patients where the clinician is intentionally treating another indication, such as depression, and where orthostasis, falls, QT/drug interactions, serotonergic combinations, next-day grogginess, and rare priapism have been considered. Other off-label sedating medications, including gabapentinoids, antipsychotics, hydroxyzine, and muscle relaxants, should not be framed as routine insomnia drugs just because they can make someone unconscious.
Plain English: trazodone is not useless, but it is not the reflex default. If the only goal is sedation, pause.
First-generation antihistamines: diphenhydramine and doxylamine
OTC is a regulatory category, not a safety guarantee.
Diphenhydramine and doxylamine are common in over-the-counter sleep aids. They can cause sedation, but they are poor repeated-use insomnia tools, especially for older adults.
Diphenhydramine has weak chronic-insomnia efficacy evidence, and its anticholinergic pharmacology is exactly the wrong direction for repeated sleep treatment, especially in older adults or anyone with cognitive vulnerability, delirium risk, urinary retention, constipation, or fall risk. Beers is a useful warning label on that biology. [5,48]
Risks: anticholinergic burden, confusion, dry mouth, constipation, urinary retention, delirium, falls, cognitive vulnerability, next-day impairment, and tolerance to the sedating effect.
Plain English: the drugstore sleep aisle is not automatically safer than the prescription pad.
Supplement decoder
Supplements are where sleep advice gets messy.
A supplement can be reasonable and still have weak evidence. It can be low risk for one person and risky for another. Product quality, dose, interactions, pregnancy or lactation, kidney or liver disease, psychiatric history, and other medications matter.
Think of supplements in four tiers.
Supplement ladder
Supplement evidence ladder
Tier 1
Best use
Context-specific tools: circadian timing, low intake or muscle tension, and subjective sleep-quality support.
Caution
Reasonable does not mean universal. Dose, timing, kidney disease, pregnancy, and interactions still matter.
Tier 2
Best use
Plausible or promising when stress, anxiety, relaxation, or mild circadian support is the dominant pattern.
Caution
Product quality and interaction risk vary. Benefits are usually conditional, not immediate knockout effects.
Tier 3
Best use
Mechanistically interesting, but not casual defaults for primary insomnia.
Caution
Serotonergic interactions, psychiatric history, THC contamination, product variability, and weak primary-insomnia evidence.
Tier 4
Best use
Generally not where I would start for chronic insomnia.
Caution
Mixed or weak evidence, side effects, quality concerns, and the risk of delaying diagnosis of the real sleep problem.
Tier 1: useful in the right context, but not miracle fixes
Melatonin
Melatonin is best understood as a circadian timing signal. It may help with delayed sleep phase, jet lag, shift work adaptation, and some older adults. It is less compelling as a generic nightly insomnia pill.
Meta-analysis suggests small average improvements in sleep latency and total sleep time, but the effect is modest and context-specific. Melatonin is strongest when the problem is circadian timing, not when the goal is chronic nightly sedation. [15]
Best use case: timing problems.
Common mistake: taking high doses at the wrong time and expecting sedation.
Safety: morning grogginess, vivid dreams, headache, interaction concerns, anticoagulants, seizure disorders, autoimmune disease, pediatric use, pregnancy or lactation, and wide dose variability in supplements.
Magnesium
Magnesium may help selected people, especially if intake is low, constipation is present, muscle tension is part of the picture, or deficiency is plausible.
A small meta-analysis in older adults suggested reduced sleep-onset latency, but certainty was low to very low and total sleep time was not clearly improved. [17]
Best use case: low magnesium intake or mild relaxation support.
Safety: diarrhea, GI upset, kidney disease caution, and medication timing interactions, including some antibiotics, thyroid medication, and bisphosphonates.
Glycine
Small RCTs using 3 g before bed suggest improvements in subjective sleep quality and some objective sleep measures. Mechanisms may include thermoregulation and sleep architecture effects. [19]
Best use case: a relatively low-risk experiment in otherwise healthy adults, assuming a quality product and no contraindications.
Safety: GI upset, pregnancy or lactation uncertainty, and clinician review for complex medical conditions.
L-theanine
L-theanine is better framed as relaxation support than as an insomnia treatment. Trials and reviews suggest possible benefit for subjective sleep quality and hyperarousal, but clinical insomnia evidence is limited.
Best use case: stress-related evening arousal without wanting heavy sedation.
Safety: additive sedation, hypotension risk in susceptible people, pregnancy or lactation uncertainty, psychiatric context, and product quality.
Tier 2: plausible or promising, but more conditional
Ashwagandha
Ashwagandha has meta-analytic RCT support for sleep improvement, with stronger signals in insomnia populations, higher doses, and longer use. [18] It is especially relevant when stress is driving sleep problems.
That said, supplement marketing tends to outrun the cautions.
Best use case: stress-related sleep difficulty in selected adults.
Safety: GI effects, sedation interactions, thyroid effects, autoimmune disease caution, pregnancy avoidance, product variability, and rare liver-injury reports.
Tart cherry
Tart cherry has small pilot data suggesting modest sleep benefits, possibly through melatonin, polyphenols, and anti-inflammatory pathways. [23]
Best use case: food-based adjunct, not a core insomnia treatment.
Safety: sugar load, GI effects, metabolic context, and dose variability.
Lavender and Silexan
Lavender aromatherapy, lavender supplements, and oral Silexan are not the same thing.
Oral Silexan has better evidence for anxiety symptoms and anxiety-related sleep disturbance than for primary insomnia. Sleep benefit may come mostly through reduced anxiety. [31-33]
Best use case: anxiety-related sleep disturbance, if the product and route are clear.
Safety: GI effects, allergy, sedation interactions, pregnancy or lactation uncertainty. Do not ingest random essential oils.
Chamomile and apigenin
Chamomile has some evidence for subjective sleep quality, but studies are heterogeneous and objective insomnia outcomes are inconsistent. Isolated apigenin supplement claims should not be treated as identical to chamomile tea evidence. [28,29]
Best use case: low-intensity relaxation ritual.
Safety: allergy risk, especially ragweed or Asteraceae sensitivity, anticoagulant concerns, pregnancy or lactation caveats, and product variability.
Tier 3: interesting, but not casual defaults
L-tryptophan and 5-HTP
Tryptophan and 5-HTP sit in the serotonin and melatonin pathway, which makes them mechanistically plausible. But plausible does not mean simple.
Tryptophan meta-analysis suggests possible reduction in wake after sleep onset, especially at doses of 1 g or more, but benefits are not broad across sleep components. Mechanistic plausibility in the serotonin/melatonin pathway is not enough to make it a chronic-insomnia default. [20]
5-HTP has small older-adult RCT data suggesting possible sleep-latency or subjective sleep-quality effects, but the evidence remains preliminary. [21]
Big safety issue: serotonergic interactions. These supplements deserve caution with SSRIs, SNRIs, MAOIs, triptans, tramadol, linezolid, MDMA, and other serotonin-raising agents unless supervised.
GABA and PharmaGABA
Oral GABA is popular. The evidence is limited. Some small studies show sleep-promoting signals, but the broader evidence base is thin and blood-brain-barrier claims are often oversold. [27]
Best use case: not a confident recommendation. At most, a cautious experiment in low-risk adults.
Safety: additive sedation, pregnancy or lactation uncertainty, and product quality.
CBD and cannabinoids
CBD is not well proven for primary insomnia. A 2024 randomized controlled pilot trial of 150 mg nightly CBD in moderate-severe insomnia did not show broad superiority to placebo across most outcomes. [26]
Cannabinoid evidence is hard to interpret because products vary by CBD dose, THC content, minor cannabinoids, route, population, and outcome.
Safety: next-day impairment, driving risk, anxiety or paranoia in some users, CYP drug interactions, liver-enzyme concerns, THC contamination or mislabeling, pregnancy or lactation avoidance, and dependence concerns with THC-containing products.
Plain English: CBD deserves a sober answer. Interesting, popular, not proven enough.
Tier 4: weak, indirect, or generally not recommended for chronic insomnia
Valerian
Valerian has mixed older evidence with methodologic concerns. That is the reason it stays low-confidence for chronic insomnia, not because a committee disliked it. [25]
Safety: sedation, interaction with alcohol and CNS depressants, liver concerns in some reports or products, and product variability.
Phosphatidylserine
Phosphatidylserine has stress and cortisol-response data, but direct insomnia evidence is weak. [30]
Best use case: maybe stress physiology research interest, not a proven sleep supplement.
Safety: GI effects, interactions, product quality, and soy sourcing or allergy depending on product.
Safety checklist before taking a sleep aid
This section should be boring. Boring safety advice prevents bad mornings, bad falls, and bad medication combinations.
Talk with a clinician before using sleep medications or sedating supplements if any of these apply:
- loud snoring, witnessed apneas, choking or gasping at night
- morning headaches, resistant hypertension, or significant daytime sleepiness
- COPD, obstructive sleep apnea, hypoventilation, obesity hypoventilation, neuromuscular disease, or opioid use
- restless legs symptoms or repetitive limb movements
- severe depression, suicidality, mania or hypomania, PTSD nightmares, panic attacks
- chronic pain, reflux, nocturia, hot flashes, thyroid symptoms, or new neurologic symptoms
- pregnancy, postpartum, lactation, or trying to conceive
- older age, frailty, cognitive impairment, delirium history, or fall risk
- liver or kidney impairment
- alcohol use, especially evening use
- use of opioids, benzodiazepines, Z-drugs, gabapentinoids, antipsychotics, muscle relaxants, sedating antihistamines, or other CNS depressants
- safety-sensitive work or driving early the next morning
Risks to say plainly
Falls and fractures: risk rises with age, nighttime bathroom trips, sedatives, antihypertensives, alcohol, frailty, and poor lighting.
Cognition and delirium: benzodiazepines, Z-drugs, anticholinergic antihistamines, and polypharmacy are the usual suspects.
Next-day impairment and driving: any hypnotic or sedating supplement can impair alertness, especially if you do not allow enough time for sleep.
Dependence, tolerance, withdrawal, rebound insomnia: most important with benzodiazepines and Z-drugs, but not limited to them.
Alcohol and CNS depressants: avoid casual combinations. Alcohol plus a sedative is not a sleep plan. It is a risk multiplier.
Respiratory risk: sedatives can be dangerous in untreated sleep apnea, COPD, hypoventilation, opioid use, and other breathing-risk states.
Pregnancy and lactation: do not assume that "natural" means safe.
Hepatic and renal impairment: metabolism and clearance matter. This affects medication choice, dose, and supplement safety.
Supplement quality: supplements can have dose variability, contamination, undeclared ingredients, heavy metals, THC contamination, or inconsistent active compounds.
Older adults: the sleep-aid aisle deserves extra caution
Many older adults are given or buy sleep aids for completely understandable reasons: grief, pain, nocturia, caregiver stress, hospitalization, anxiety, or years of fragmented sleep.
But this is also the group where harm shows up fastest.
The highest-concern repeated-use choices are:
- benzodiazepines
- Z-drugs
- diphenhydramine
- doxylamine
- high-dose doxepin above 6 mg/day
- combinations of sedating medications
- alcohol plus any sedative
The harms are not theoretical. Falls, fractures, delirium, confusion, urinary retention, constipation, next-day impairment, and car accidents change lives.
If an older adult is suddenly sleeping worse, look for causes before escalating sedation: pain, infection, urinary symptoms, constipation, medication changes, alcohol, depression, cognitive change, sleep apnea, restless legs, and environmental disruption.
Longevity framing: sleep matters, but sleep drugs are not longevity drugs
Sleep is a core health input. Poor sleep and chronic insomnia are associated with cardiometabolic risk, blood pressure dysregulation, mood symptoms, pain sensitivity, immune changes, cognitive risk, and accidents. Sleep regularity and sleep architecture are increasingly important in the aging conversation.
So yes, sleep belongs in longevity medicine.
But no sleep medication should be marketed as a longevity drug.
Better sleep may support better long-term health. A medication that increases sedation is not automatically improving healthspan. A supplement that nudges sleep latency by a few minutes is not an anti-aging therapy. A wearable-reported increase in deep sleep is not proof of brain clearance, dementia prevention, or biological-age reversal.
The most credible longevity framing is simple:
- Protect sleep opportunity.
- Stabilize circadian timing.
- Treat insomnia with CBT-I when it becomes chronic.
- Screen for sleep apnea and other medical causes when the pattern suggests it.
- Use medications selectively, with safety and daytime function in mind.
- Treat supplements as optional adjuncts, not the foundation.
DORA Alzheimer biomarker research is worth watching. It is not prevention evidence. The honest sentence is: short-term biomarker changes are interesting, and long-term clinical outcomes are unproven. [13]
A practical way to choose the next step
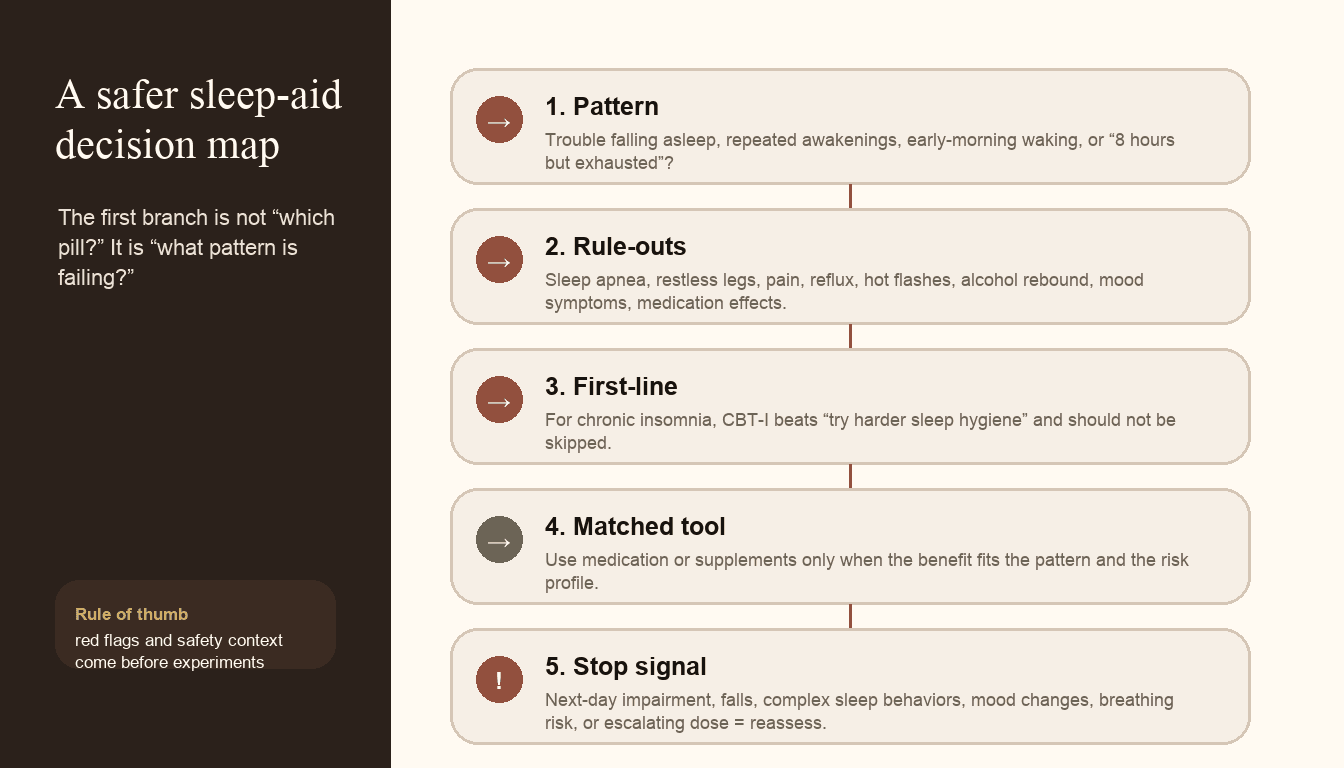
The safer sleep-aid question is pattern first, tool second.
If you are trying to decide what to do tonight, start here.
If the problem is trouble falling asleep
Think first about:
- caffeine timing
- evening light
- delayed circadian phase
- inconsistent wake time
- stress or conditioned arousal
- late exercise
- alcohol
Possible tools to discuss with a clinician: CBT-I, circadian light timing, melatonin timing, ramelteon, selected short-term hypnotic use only when appropriate.
If the problem is waking up repeatedly
Think first about:
- sleep apnea
- alcohol rebound
- pain
- hot flashes
- nocturia
- restless legs
- reflux
- medication effects
- hyperarousal
Possible tools to discuss with a clinician: CBT-I, evaluation for sleep apnea or restless legs, menopause treatment when relevant, low-dose doxepin, DORAs, and targeted treatment of the underlying driver.
If the problem is waking too early
Think first about:
- depression or mood symptoms
- circadian phase advance
- alcohol
- stress physiology
- sleep schedule mismatch
- pain or hot flashes
Possible tools to discuss with a clinician: CBT-I, light timing, mood evaluation, low-dose doxepin or DORA in selected cases, and treatment of the actual driver.
If the problem is "I sleep 8 hours and wake exhausted"
Do not just add a sleep aid.
Think first about:
- obstructive sleep apnea
- insufficient deep sleep or fragmented sleep
- periodic limb movements
- alcohol
- medications
- depression
- chronic pain
- thyroid disease
- iron deficiency or restless legs
This is a "get evaluated" pattern, especially if there is snoring, gasping, morning headache, hypertension, or daytime sleepiness.
What I would not do
I would not use alcohol as a sleep aid.
I would not use diphenhydramine or doxylamine nightly and call it harmless because it is OTC.
I would not stack multiple sedatives or sedating supplements without a clinician reviewing the full list.
I would not treat untreated sleep apnea with a stronger hypnotic.
I would not call melatonin a sleeping pill.
I would not tell an older adult to "just take Benadryl."
I would not market DORAs as dementia prevention.
And I would not confuse being knocked out with getting well.
Sources and method
This guide uses guidelines as secondary summaries, not as authority endpoints. The hierarchy is: mechanisms, clinical endpoints, randomized trials, PSG/EEG architecture studies, systematic reviews, meta-analyses, FDA safety communications, prescribing information, and then guideline statements as a check on interpretation. The evidence is intentionally presented by use case and risk profile rather than as a universal ranking of “best sleep aids.”
The practical hierarchy is:
- behavioral treatment and diagnosis of the sleep pattern first;
- medication only when matched to the phenotype and safety context;
- supplements as optional, modest, quality-dependent adjuncts;
- urgent caution around older adults, respiratory risk, sedative stacking, alcohol, pregnancy/lactation, driving, and cognitive/fall risk.
Clinical lens
How I’d decide
Use this section as a second pass after the main answer, not as homework before you know what the page is saying.
Who it’s for
Adults trying to understand insomnia medications, melatonin, magnesium, CBD, OTC sleep aids, and sleep supplements through an evidence-and-safety lens.
Who should skip it
Do not self-treat persistent insomnia if you have suspected sleep apnea, restless legs, severe mood symptoms, pregnancy or lactation, COPD or hypoventilation risk, opioid or alcohol use, fall risk, cognitive symptoms, or complex medication interactions.
Measure before / after
Track the actual pattern: sleep onset, awakenings, early-morning waking, total sleep time, sleep efficiency, next-day alertness, snoring or breathing symptoms, alcohol/caffeine timing, naps, and medication/supplement side effects.
What I’d do first
I would start by defining the sleep phenotype, ruling out non-insomnia drivers, using CBT-I for chronic insomnia, and then considering targeted medication or supplement options only when the benefit matches the risk context.
What would change my mind
Escalating dose, next-day impairment, falls, complex sleep behaviors, mood changes, worsening breathing symptoms, or persistent unrefreshing sleep should change the plan and trigger reassessment.
Frequently Asked Questions
Are sleep medications the same as natural sleep?
No. Some medications can help insomnia, but sedation is not the same as physiologic sleep. Restorative sleep has architecture, timing, continuity, and stable breathing. A medication that reduces awareness does not automatically restore those features.
What is the best first treatment for chronic insomnia?
CBT-I has the strongest durable evidence for chronic insomnia because randomized trials and meta-analyses show improvements in insomnia severity, sleep efficiency, sleep latency, and wake after sleep onset without the same tolerance, dependence, or interaction logic as sedative drugs. Sleep hygiene helps, but CBT-I is the structured treatment: stimulus control, sleep restriction or compression, cognitive work, relaxation, and circadian regularity.
Are DORAs safer than Ambien?
DORAs work differently from Z-drugs like zolpidem. They reduce orexin wake signaling rather than primarily enhancing GABAergic sedation. That may be a better physiology match for some patients, but it does not make them risk-free. DORAs can still cause next-day impairment, complex sleep behaviors, mood cautions, additive sedation, and breathing-risk concerns.
Is trazodone a good sleep medication?
Trazodone can make people sleepy and may reduce awakenings in some studies, but it is an off-label antidepressant rather than a first-line chronic-insomnia treatment. The evidence is mixed/modest, sleep-architecture changes do not prove long-term brain benefit, and risks include orthostatic hypotension, dizziness, next-day impairment, QT or drug-interaction concerns, serotonergic interactions, falls, and rare priapism.
Is melatonin a sleeping pill?
Not really. Melatonin is better understood as a circadian timing signal. It can help with jet lag, delayed sleep phase, and timing problems. Its average effect for chronic insomnia is modest, and higher doses are not automatically better.
Is magnesium good for sleep?
Magnesium may help some people, especially if intake is low or deficiency is plausible. The evidence is modest and not universal. It can cause GI side effects and needs caution in kidney disease and with some medication timing.
Does CBD work for insomnia?
CBD is not well proven for primary insomnia. Early trials are mixed, and products vary widely. Safety issues include next-day impairment, drug interactions, liver-enzyme concerns, THC contamination, pregnancy or lactation concerns, and driving risk.
Are OTC sleep aids safe?
Not necessarily. Diphenhydramine and doxylamine can cause anticholinergic side effects, next-day impairment, urinary retention, constipation, confusion, delirium, and falls, especially in older adults.
What sleep aid is safest for older adults?
There is no universal safest sleep aid. The safer first step is to identify why sleep is disrupted. Pain, nocturia, sleep apnea, restless legs, depression, medication changes, alcohol, and environmental disruption are common. Older adults should be especially cautious with benzodiazepines, Z-drugs, diphenhydramine, doxylamine, high-dose doxepin, and medication stacking.
Can sleep medications prevent dementia?
No sleep medication should be described as dementia prevention. DORAs have interesting early biomarker data, but biomarker changes are not the same as long-term prevention of Alzheimer disease or cognitive decline.
When should insomnia trigger medical evaluation?
Get evaluated if insomnia is persistent, worsening, associated with loud snoring or gasping, significant daytime sleepiness, morning headaches, resistant hypertension, restless legs, depression, mania, panic, trauma symptoms, chronic pain, hot flashes, nocturia, medication changes, alcohol use, pregnancy, cognitive symptoms, or breathing disease.
References & citations
- 1.Brown EN, Lydic R, Schiff ND. General anesthesia, sleep, and coma. N Engl J Med. 2010;363(27):2638-2650. DOI: 10.1056/NEJMra0808281. PMID: 21190458.
- 2.Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, et al. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: an American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(2):307-349. DOI: 10.5664/jcsm.6470. PMID: 27998379.
- 3.Edinger JD, Arnedt JT, Bertisch SM, Carney CE, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021;17(2):255-262. DOI: 10.5664/jcsm.8986. PMID: 33164742.
- 4.Qaseem A, Kansagara D, Forciea MA, Cooke M, et al. Management of Chronic Insomnia Disorder in Adults: a Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016;165(2):125-133. DOI: 10.7326/M15-2175. PMID: 27136449.
- 5.American Geriatrics Society 2023 updated AGS Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2023;71(7):2052-2081. DOI: 10.1111/jgs.18372. PMID: 37139824.
- 6.FDA. Certain Prescription Insomnia Medicines: new boxed warning due to risk of serious injuries caused by complex sleep behaviors. 2019.
- 7.Harbourt K, Nevo ON, Zhang R, Chan V, et al. Association of eszopiclone, zaleplon, or zolpidem with complex sleep behaviors resulting in serious injuries, including death. Pharmacoepidemiol Drug Saf. 2020;29(6):684-691. DOI: 10.1002/pds.5004. PMID: 32323442.
- 8.DailyMed. BELSOMRA, suvorexant prescribing information.
- 9.DailyMed. DAYVIGO, lemborexant prescribing information.
- 10.DailyMed. QUVIVIQ, daridorexant prescribing information.
- 11.Rosenberg R, Murphy P, Zammit G, Mayleben D, et al. Comparison of lemborexant with placebo and zolpidem tartrate extended release for the treatment of older adults with insomnia disorder: a phase 3 randomized clinical trial. JAMA Netw Open. 2019;2(12):e1918254. DOI: 10.1001/jamanetworkopen.2019.18254. PMID: 31880796.
- 12.Mignot E, Mayleben D, Fietze I, Leger D, et al. Safety and efficacy of daridorexant in patients with insomnia disorder: results from two multicentre, randomized, double-blind, placebo-controlled, phase 3 trials. Lancet Neurol. 2022;21(2):125-139. DOI: 10.1016/S1474-4422(21)00436-1. PMID: 35065036.
- 13.Lucey BP, Liu H, Toedebusch CD, Freund D, et al. Suvorexant acutely decreases tau phosphorylation and amyloid-beta in the human CNS. Ann Neurol. 2023;94(1):27-40. DOI: 10.1002/ana.26641. PMID: 36897120.
- 14.Yeung WF, Chung KF, Yung KP, Ng TH. Doxepin for insomnia: a systematic review of randomized placebo-controlled trials. Sleep Med Rev. 2015;19:75-83. DOI: 10.1016/j.smrv.2014.06.001. PMID: 25047681.
- 15.Ferracioli-Oda E, Qawasmi A, Bloch MH. Meta-analysis: melatonin for the treatment of primary sleep disorders. PLoS One. 2013;8(5):e63773. DOI: 10.1371/journal.pone.0063773. PMID: 23691095.
- 16.Kuriyama A, Honda M, Hayashino Y. Ramelteon for the treatment of insomnia in adults: a systematic review and meta-analysis. Sleep Med. 2014;15(4):385-392. DOI: 10.1016/j.sleep.2013.11.788. PMID: 24656909.
- 17.Mah J, Pitre T. Oral magnesium supplementation for insomnia in older adults: a systematic review and meta-analysis. BMC Complement Med Ther. 2021;21(1):125. DOI: 10.1186/s12906-021-03297-z. PMID: 33865376.
- 18.Cheah KL, Norhayati MN, Husniati Yaacob L, Abdul Rahman R. Effect of Ashwagandha extract on sleep: a systematic review and meta-analysis. PLoS One. 2021;16(9):e0257843. DOI: 10.1371/journal.pone.0257843. PMID: 34559859.
- 19.Yamadera W, Inagawa K, Chiba S, et al. Glycine ingestion improves subjective sleep quality in human volunteers, correlating with polysomnographic changes. Sleep Biol Rhythms. 2007. DOI: 10.1111/j.1479-8425.2007.00262.x.
- 20.Sutanto CN, Loh WW, Kim JE. The impact of tryptophan supplementation on sleep quality: a systematic review, meta-analysis, and meta-regression. Nutr Rev. 2022;80(2):306-316. DOI: 10.1093/nutrit/nuab027. PMID: 33942088.
- 21.Sutanto CN, Xia X, Heng CW, Tan YS, et al. The impact of 5-hydroxytryptophan supplementation on sleep quality and gut microbiota composition in older adults: a randomized controlled trial. Clin Nutr. 2024;43(3):593-602. DOI: 10.1016/j.clnu.2024.01.010. PMID: 38309227.
- 22.Cotter J, Caddick CE, Harper JL, Ebajemito JK. Examining the effect of L-theanine on sleep: a systematic review of dietary supplementation trials. Nutr Neurosci. 2026;29(2):224-238. DOI: 10.1080/1028415X.2025.2556925. PMID: 41176609.
- 23.Pigeon WR, Carr M, Gorman C, Perlis ML. Effects of a tart cherry juice beverage on the sleep of older adults with insomnia: a pilot study. J Med Food. 2010;13(3):579-583. DOI: 10.1089/jmf.2009.0096. PMID: 20438325.
- 24.Monoi N, Matsuno A, Nagamori Y, Kimura E, et al. Japanese sake yeast supplementation improves the quality of sleep: a double-blind randomized controlled clinical trial. J Sleep Res. 2016;25(1):116-123. DOI: 10.1111/jsr.12336. PMID: 26354605.
- 25.Bent S, Padula A, Moore D, Patterson M, et al. Valerian for sleep: a systematic review and meta-analysis. Am J Med. 2006;119(12):1005-1012. DOI: 10.1016/j.amjmed.2006.02.026. PMID: 17145239.
- 26.Narayan AJ, Downey LA, Rose S, Di Natale L, et al. Cannabidiol for moderate-severe insomnia: a randomized controlled pilot trial of 150 mg of nightly dosing. J Clin Sleep Med. 2024;20(5):753-763. DOI: 10.5664/jcsm.10998. PMID: 38174873.
- 27.Yoon S, Byun JI, Shin WC. Efficacy and safety of low-dose gamma-aminobutyric acid from unpolished rice germ as a health functional food for promoting sleep: a randomized, double-blind, placebo-controlled trial. J Clin Neurol. 2022;18(4):478-480. DOI: 10.3988/jcn.2022.18.4.478. PMID: 35796273.
- 28.Kazemi A, Shojaei-Zarghani S, Eskandarzadeh P, Hashempur MH. Effects of chamomile on sleep: a systematic review and meta-analysis of clinical trials. Complement Ther Med. 2024;84:103071. DOI: 10.1016/j.ctim.2024.103071. PMID: 39106912.
- 29.Hieu TH, Dibas M, Surya Dila KA, Sherif NA, et al. Therapeutic efficacy and safety of chamomile for state anxiety, generalized anxiety disorder, insomnia, and sleep quality: a systematic review and meta-analysis of randomized trials and quasi-randomized trials. Phytother Res. 2019;33(6):1604-1615. DOI: 10.1002/ptr.6349. PMID: 31006899.
- 30.Hellhammer J, Hero T, Franz N, Contreras C, et al. A soy-based phosphatidylserine/phosphatidic acid complex normalizes stress reactivity of the hypothalamus-pituitary-adrenal axis in chronically stressed male subjects: a randomized, placebo-controlled study. Lipids Health Dis. 2014;13:121. DOI: 10.1186/1476-511X-13-121.
- 31.Seifritz E, Kasper S, Möller HJ, Volz HP, et al. Effect of anxiolytic drug Silexan on sleep: a narrative review. World J Biol Psychiatry. 2022;23(7):493-500. DOI: 10.1080/15622975.2021.2013092. PMID: 36259937.
- 32.Greenberg MJ, Slyer JT. Effectiveness of Silexan oral lavender essential oil compared to inhaled lavender essential oil aromatherapy for sleep in adults: a systematic review. JBI Database System Rev Implement Rep. 2018. PMID: 30439747. DOI: 10.11124/JBISRIR-2017-003823.
- 33.Hwang E, Shin S. The effect of lavender on sleep quality in individuals without insomnia: a systematic review. J Altern Complement Med. 2022. PMID: 35708558.
- 34.Roth AJ, McCall WV, Liguori A. Cognitive, psychomotor and polysomnographic effects of trazodone in primary insomniacs. J Sleep Res. 2011;20(4):552-558. DOI: 10.1111/j.1365-2869.2011.00928.x. PMID: 21623982.
- 35.Yi XY, Ni SF, Ghadami MR, et al. Trazodone for the treatment of insomnia: a meta-analysis of randomized placebo-controlled trials. Sleep Med. 2018;45:25-32. DOI: 10.1016/j.sleep.2018.01.010. PMID: 29680424.
- 36.Kokkali M, Pinioti E, Lappas AS, et al. Effects of Trazodone on Sleep: A Systematic Review and Meta-analysis. CNS Drugs. 2024;38(10):753-769. DOI: 10.1007/s40263-024-01110-2. PMID: 39123094.
- 37.Zheng Y, Lv T, Wu J, Lyu Y. Trazodone changed the polysomnographic sleep architecture in insomnia disorder: a systematic review and meta-analysis. Sci Rep. 2022;12(1):14453. DOI: 10.1038/s41598-022-18776-7. PMID: 36002579.
- 38.Herring WJ, Connor KM, Ivgy-May N, et al. Suvorexant in Patients With Insomnia: Results From Two 3-Month Randomized Controlled Clinical Trials. Biol Psychiatry. 2016;79(2):136-148. DOI: 10.1016/j.biopsych.2014.10.003. PMID: 25526970.
- 39.Snyder E, Ma J, Svetnik V, et al. Effects of suvorexant on sleep architecture and power spectral profile in patients with insomnia: analysis of pooled phase 3 data. Sleep Med. 2016;19:93-100. DOI: 10.1016/j.sleep.2015.10.007. PMID: 27198953.
- 40.Moline M, Zammit G, Cheng JY, et al. Comparison of the effect of lemborexant with placebo and zolpidem tartrate extended release on sleep architecture in older adults with insomnia disorder. J Clin Sleep Med. 2021;17(6):1167-1174. DOI: 10.5664/jcsm.9150. PMID: 33590823.
- 41.Di Marco T, Djonlagic I, Dauvilliers Y, et al. Effect of daridorexant on sleep architecture in patients with chronic insomnia disorder: a pooled post hoc analysis of two randomized phase 3 clinical studies. Sleep. 2024;47(11):zsae098. DOI: 10.1093/sleep/zsae098. PMID: 38644625.
- 42.Rocha RB, Bomtempo FF, Nager GB, et al. Dual orexin receptor antagonists for the treatment of insomnia: systematic review and network meta-analysis. Arq Neuropsiquiatr. 2023;81(5):475-483. DOI: 10.1055/s-0043-1768667. PMID: 37257468.
- 43.Na HJ, Jeon N, Staatz CE, et al. Clinical safety and narcolepsy-like symptoms of dual orexin receptor antagonists in patients with insomnia: a systematic review and meta-analysis. Sleep. 2024;47(2):zsad293. DOI: 10.1093/sleep/zsad293. PMID: 37950346.
- 44.Kishi T, Ikuta T, Citrome L, et al. Comparative efficacy and safety of daridorexant, lemborexant, and suvorexant for insomnia: a systematic review and network meta-analysis. Transl Psychiatry. 2025;15(1):211. DOI: 10.1038/s41398-025-03439-8. PMID: 40555730.
- 45.Trauer JM, Qian MY, Doyle JS, Rajaratnam SMW, Cunnington D. Cognitive Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-analysis. Ann Intern Med. 2015;163(3):191-204. DOI: 10.7326/M14-2841. PMID: 26054060.
- 46.Brasure M, Fuchs E, MacDonald R, Nelson VA, Koffel E, Olson CM, et al. Psychological and Behavioral Interventions for Managing Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165(2):113-124. DOI: 10.7326/M15-1782. PMID: 27136619.
- 47.van Straten A, van der Zweerde T, Kleiboer A, Cuijpers P, Morin CM, Lancee J. Cognitive and behavioral therapies in the treatment of insomnia: a meta-analysis. Sleep Med Rev. 2018;38:3-16. DOI: 10.1016/j.smrv.2017.02.001. PMID: 28392168.
- 48.Wilt TJ, MacDonald R, Brasure M, Olson CM, Carlyle M, Fuchs E, Khawaja IS, et al. Pharmacologic Treatment of Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165(2):103-112. DOI: 10.7326/M15-1781. PMID: 27136278.
Related Guides
Next step
Turn the guide into the right next decision.
If this page raised a real clinical question, start with the practice details. If you are still learning, get the weekly letter. If you are comparing tests, use the testing hub before buying another panel.