A new aging mechanism puts iron on trial, and it matters even if you never bought an iron pill.
There is a supplement millions of people take without meaning to.
Not because it is trendy. Because it feels responsible.
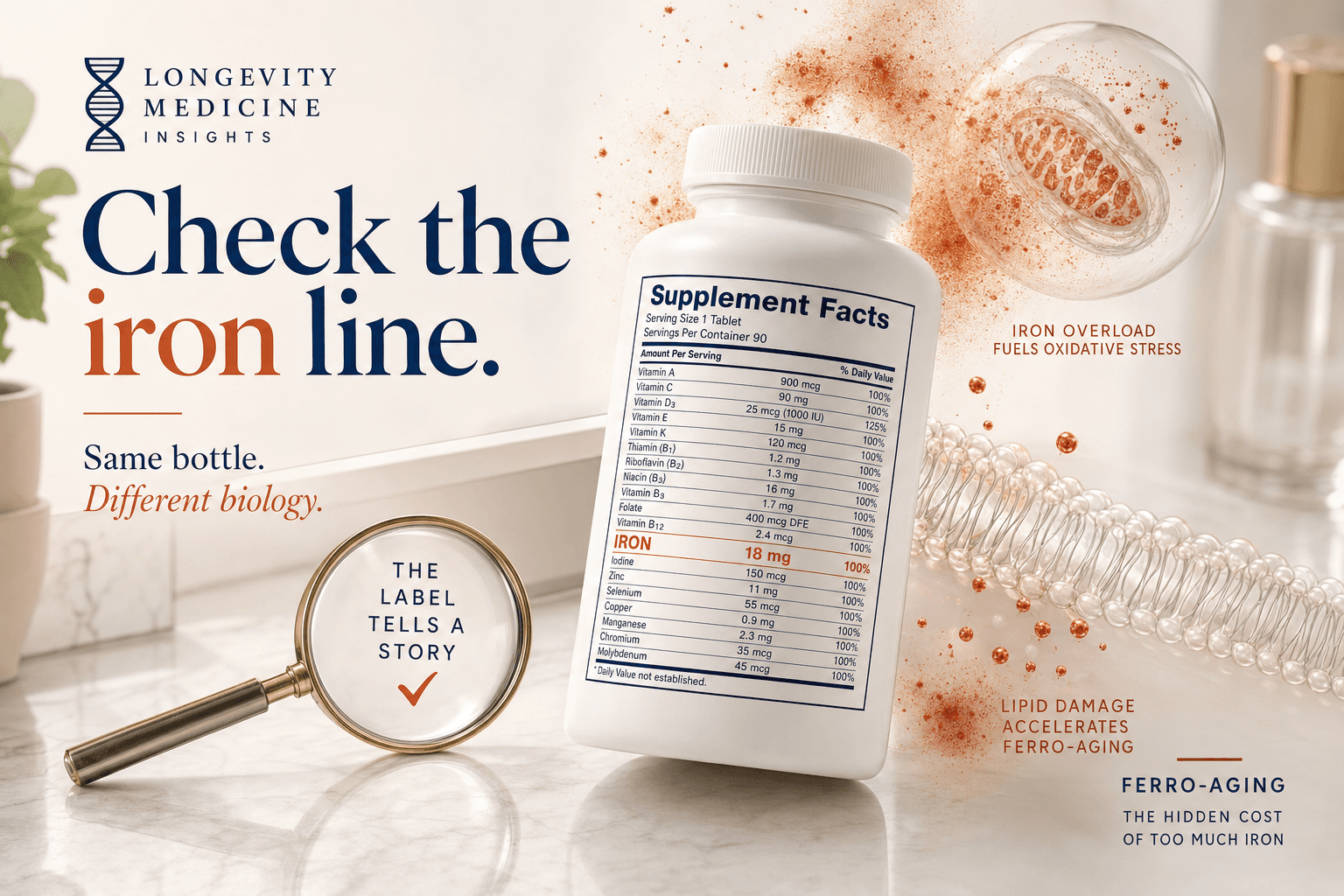
It is tucked into multivitamins, prenatals, “energy” formulas, fortified foods, and tiny Supplement Facts panels nobody reads because nobody enjoys medical hide-and-seek.
The supplement is iron.
If you are truly deficient, iron can be life-changing. Pregnancy, heavy periods, blood loss, malabsorption, anemia: iron may be exactly what you need.
But if you are a man, a post-menopausal woman, someone who does not menstruate, or anyone taking iron only because it came bundled inside a generic multi, pause.
A new Cell Metabolism paper names ferro-aging, a slow iron-lipid damage pathway that builds up in aging tissues.
Now the weird part: vitamin C.
Not as an “immune booster.” Not as a reason to start megadosing.
Yes, vitamin C is an antioxidant. That matters here because ferro-aging is partly about oxidative damage to fatty cell membranes. But the interesting part of this paper is more specific than “antioxidants good.”
Vitamin C appears to inhibit ACSL4, an enzyme that can make cell membranes more vulnerable to iron-driven damage. So there are two ideas sitting next to each other: vitamin C may help buffer oxidative stress, and it may also affect one of the enzymes that helps set up iron-driven lipid damage in the first place.
But that brings us back to the boring, useful question: why are you taking iron in the first place?
If your multivitamin has iron, your ferritin is weird, or someone once told you to “just take iron,” don’t skip the protocol at the end. The whole decision may come down to one tiny line on the label.
TL;DR
🧲 The Deep Dive: Why iron is essential, and why too much or misplaced iron can become oxidative membrane damage.
🐒 The New Study: The primate data that make ferro-aging more than a cell-culture story.
🍊 Vitamin C: Why it is suddenly interesting again, beyond the usual “antioxidants good” story.
💊 Hidden Iron: How iron sneaks in even if you never bought an iron supplement.
🧪 The Protocol: The lab panel and bottle-label check I would actually use before taking iron.
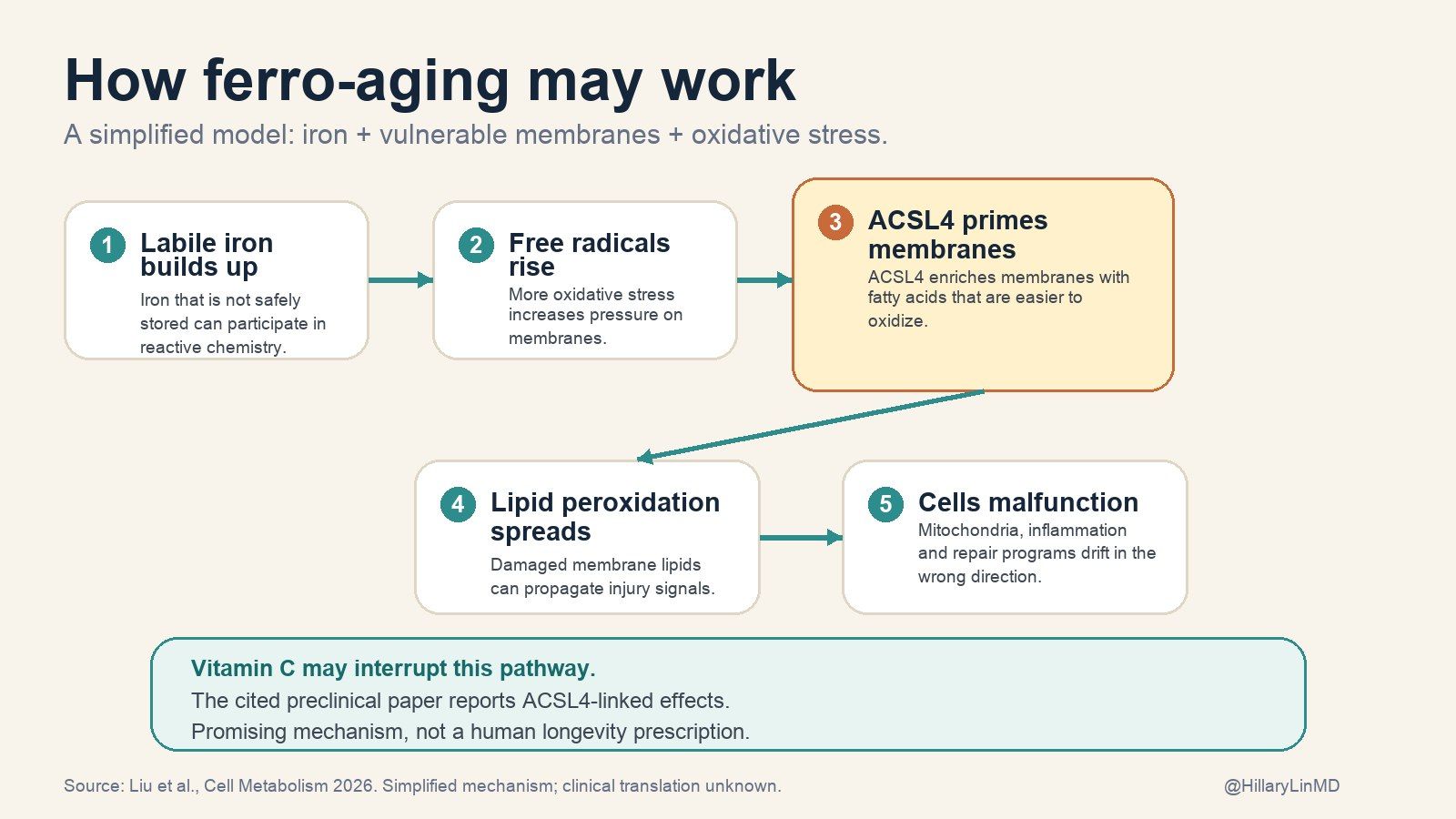
Ferro-aging, simplified. Iron can fuel lipid peroxidation, ACSL4 appears to make membranes more vulnerable, and vitamin C may interrupt the pathway. Promising preclinical mechanism, not proof that vitamin C reverses aging in humans.
Iron does not just “give you energy”
Iron is powerful because it can move electrons.
That is why your body needs it for oxygen transport, mitochondrial function, and many enzymes.
It is also why excess or misplaced iron can drive oxidative damage. A review of iron, cardiovascular disease, and diabetes makes the same basic point: iron biology shows up across chronic disease because free iron is chemically reactive.
In the ferro-aging model, aging tissues accumulate iron. That iron fuels lipid peroxidation, which is damage to the fatty membranes surrounding cells and organelles.
ACSL4 seems to amplify the problem by loading membranes with oxidation-prone polyunsaturated fats. In plain English: it helps choose the kind of material your cell membranes are built from, and some of that material is easier for iron to damage.
This is related to ferroptosis, the acute iron-dependent cell death pathway studied in cancer and neurodegeneration.
But ferro-aging is slower. The cells do not necessarily die right away. They become worse at their jobs: more dysfunctional, more senescent, more inflammatory.
Honestly, rude.
The primate data are why this is worth reading
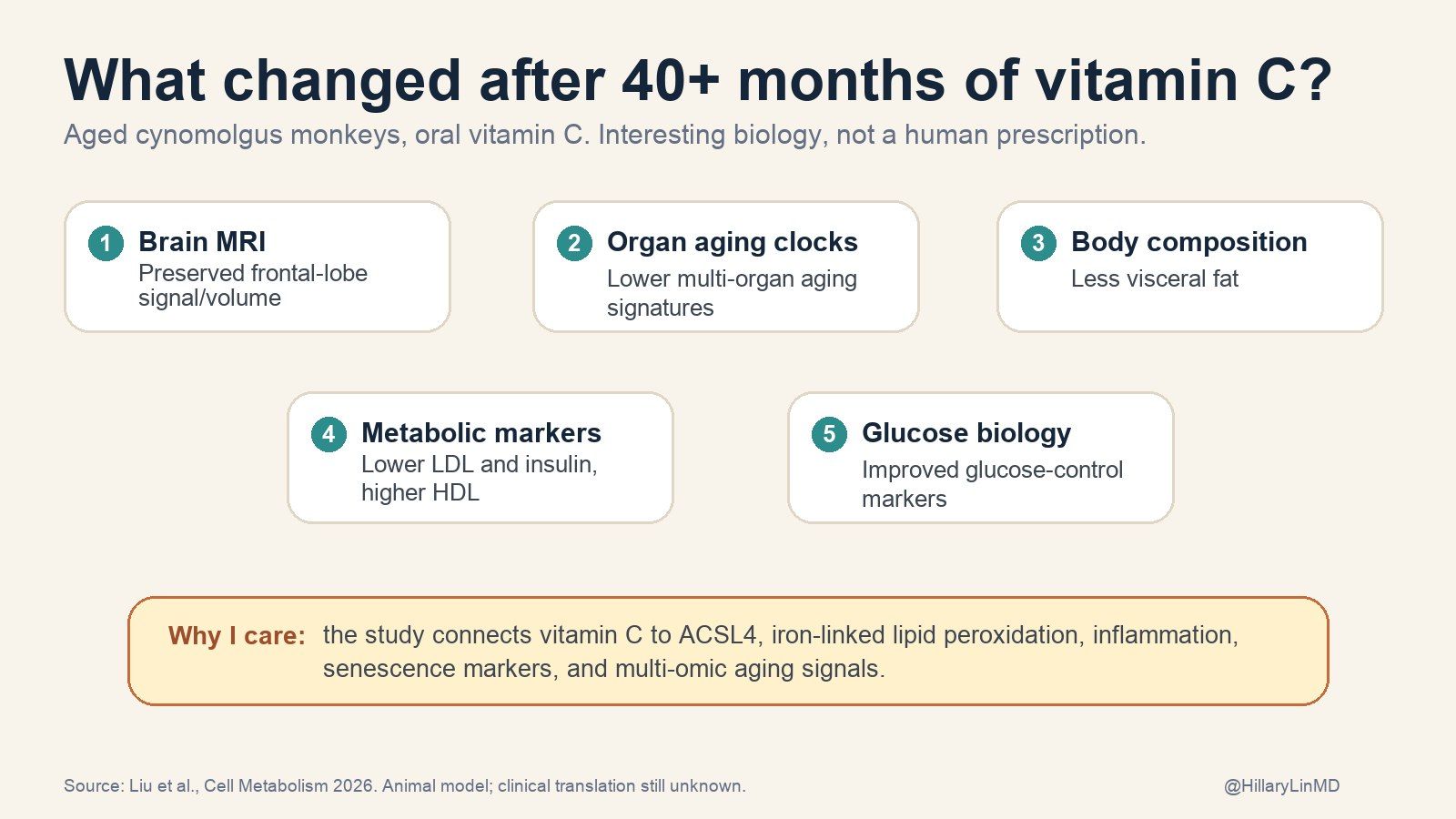
The new paper is worth attention because it combines human tissue data, non-human primate tissue data, mouse experiments, compound screening, and a long-term vitamin C intervention in aged cynomolgus monkeys.
The authors report:
Aging tissues showed more iron accumulation and lipid peroxidation. This appeared across multiple tissues.
ACSL4 rose with age and helped drive the damage pattern. Inhibiting hepatic ACSL4 in old mice improved several aging-associated phenotypes.
Vitamin C emerged as a direct ACSL4 inhibitor. That is the part that made me do a double-take.
Aged monkeys treated with vitamin C for more than 40 months showed lower ferro-aging signatures. They also had improvements in oxidative stress, inflammation, senescence markers, metabolic markers, brain MRI signals, and multi-omic aging clocks.
That is stronger than a mouse-only longevity claim.
It is also exactly the kind of paper that can become a supplement ad by Tuesday.
It is still not a human outcomes trial.
We do not know whether vitamin C supplementation in humans prevents dementia, reduces heart attacks, preserves muscle, or extends life through ACSL4 inhibition. We also do not know the ideal dose, formulation, or who benefits most.
This is exactly where the wellness internet usually swerves into a shopping cart.
I would rather use the paper for a cleaner clinical lesson: iron and vitamin C are not background noise. They are aging-relevant biology.
The primate data are why this paper got my attention. But “promising primate biology” is not the same as a human prescription.
The vitamin C paper is the doorway
The reason I care about this is not “new paper says vitamin C did something in monkeys.”
Iron keeps showing up in the biology of aging and chronic disease:
Brain aging: A review called “The Aging of Iron Man” describes brain iron dyshomeostasis as a recurring feature of aging and neurodegenerative disease, tied to oxidative stress, neuroinflammation, protein aggregation, mitochondrial dysfunction, and cognitive decline.
The iron-lipid loop: A neurodegeneration review describes a vicious cycle where lipid peroxidation and iron accumulation can reinforce each other through mitochondria, lysosomes, autophagy, lipofuscin, and ferroptosis pathways.
Metabolic and vascular disease: Iron status has been studied in cardiovascular disease, diabetes, insulin resistance, and LDL oxidation. The evidence is too messy for a slogan like “lower iron equals longer life.” It is not too messy to say iron is not a passive mineral sitting quietly in the background.
Cancer biology: Cancer cells often rewire iron metabolism because rapidly dividing cells need iron. That is part of why ferroptosis is being studied as a cancer vulnerability. Same chemistry, very different clinical question.
So no, do not panic about iron.
Just stop treating it like a harmless default ingredient.
“But I do not take iron.” Are you sure?
This is the point where many readers think: fine, but I do not take an iron supplement.
Maybe. But check.
Iron can show up in:
Multivitamins
Prenatals
“Women’s energy” formulas
Fortified cereals and grains
Meal replacements
Protein powders
Some “hair, skin, nails” products
The Supplement Facts label is annoying and tiny because apparently bottle designers want us all to suffer. Still, look. The line you want may simply say Iron or Ferrous fumarate / sulfate / gluconate / bisglycinate.
And even if you do not supplement iron, iron status can shift because of age, diet, inflammation, menstruation, menopause, alcohol intake, fatty liver, and genetics.
The question is not “is iron good or bad?”
The question is: what is your iron economy doing?
The questions that change the answer
What if I eat a lot of red meat?
Red meat contains heme iron, which is generally absorbed more efficiently than plant-based non-heme iron. That does not mean red meat automatically causes iron overload. It means it can matter more in someone already trending high.
If you eat a lot of red meat and you are a man or post-menopausal woman, I would be more interested in checking ferritin and transferrin saturation than arguing abstractly about meat. One large NIH-AARP pancreatic cancer analysis found higher risk signals with red meat, high-temperature cooking, and heme iron from red meat, especially in men. The lab pattern is still more useful than the food fight.
What if I am plant-based?
Plant-based eaters are often more likely to run low, especially if menstrual losses are heavy or intake is inconsistent. Non-heme iron from plants is less efficiently absorbed, and absorption is affected by phytates, tea, coffee, calcium, and meal composition.
For a plant-based person with low ferritin, vitamin C with meals can be useful because it increases non-heme iron absorption.
Context, context, context. Medicine’s least sexy but most reliable word.
Wait, is vitamin C just acting as an antioxidant?
Partly, probably. Vitamin C is a water-soluble antioxidant, and ferro-aging involves oxidative damage to lipids in cell membranes. So the basic antioxidant story is relevant.
But the reason this paper is interesting is that it does not stop there. The authors also identify vitamin C as a direct inhibitor of ACSL4, the enzyme that helps load membranes with fats that are more vulnerable to iron-driven peroxidation.
A simple way to say it: vitamin C may help clean up oxidative stress, but it may also help make the membrane less flammable in the first place.
That does not turn vitamin C into a magic longevity drug. It just makes the mechanism less hand-wavy than the usual “take antioxidants” advice.
Wait, does vitamin C increase iron absorption? Is that safe?
Yes, vitamin C can increase absorption of non-heme iron. That is helpful if you are deficient.
If you have iron overload, hereditary hemochromatosis, high transferrin saturation, or you are taking high-dose iron without an indication, that same effect deserves caution.
This is why I do not love blanket rules like “take vitamin C with every iron-containing meal.” Good advice for one person can be the wrong advice for another.
Can this relate to cancer?
Possibly, but carefully.
Iron, lipid peroxidation, ACSL4, and ferroptosis are all active areas in cancer biology. A review on ACSL3, ACSL4, ferroptosis, and cancers describes ACSL4 as part of the machinery that can make cells more ferroptosis-sensitive.
A newer population-evidence review on iron and cancer is useful here too: heme iron is more consistently associated with cancer risk than non-heme iron, but the biomarker data are messy and cancer-type specific.
That does not mean vitamin C is a cancer treatment. It does not mean iron causes cancer in a simple one-step way. Cancer biology is not a motivational quote, despite everyone’s best efforts on the internet.
It does mean the iron-lipid damage pathway sits near biology that cancer researchers care about. That makes it more interesting, not clinically settled.
What else raises ferritin besides iron overload?
A lot.
Ferritin rises with inflammation, infection, liver injury, alcohol use, fatty liver, metabolic dysfunction, some malignancies, and chronic disease. A high ferritin can mean iron overload. It can also mean your immune system or liver is waving a flag.
That is why ferritin alone is not enough.
Ferritin is useful. It is not a verdict.
Ferritin is the iron storage marker most people know.
Low ferritin can identify depleted iron stores before anemia is obvious. High ferritin can suggest excess iron stores, but it can also rise for reasons that are not primarily iron overload.
This is not just theoretical nitpicking. In an NHANES III mortality follow-up, ferritin was not independently associated with all-cause, cancer, or cardiovascular mortality in older men or post-menopausal women. That does not make ferritin useless. It means ferritin alone is too blunt for longevity conclusions.
The marker I do not want people skipping is transferrin saturation.
Transferrin is the main iron transport protein in blood. Transferrin saturation tells you what percentage of those binding sites are occupied by iron. A repeatedly high transferrin saturation, especially with high ferritin, raises a different concern than ferritin alone.
That is when I start thinking about iron-loading states, including hereditary hemochromatosis, and repeating the test rather than reacting to one weird lab in isolation.
The pattern matters:
Low ferritin + low transferrin saturation: often true deficiency.
High ferritin + high transferrin saturation: think iron overload pattern.
High ferritin + normal/low transferrin saturation + high hs-CRP or abnormal liver enzymes: think inflammation, liver/metabolic context, or mixed picture.
Same molecule. Different patient. Opposite decision.
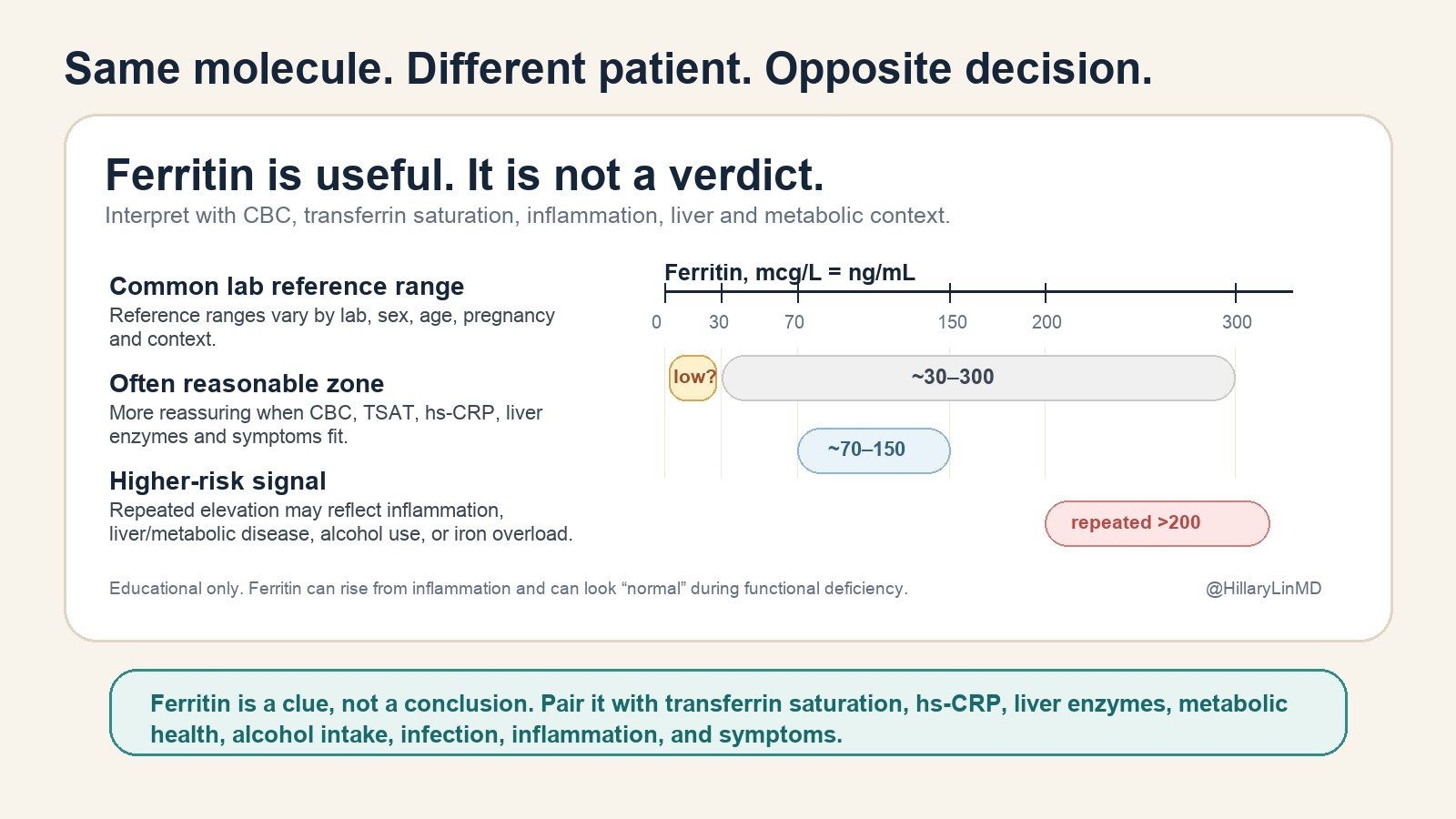
Ferritin is useful, but it is not a standalone verdict. Interpret it with transferrin saturation, hs-CRP, liver enzymes, metabolic health, alcohol intake, infection, inflammation, and symptoms.
The lab panel I would actually check
If you are taking iron, thinking about iron, or taking a multivitamin that contains it, I would want more than vibes.
I would usually check:
Ferritin: storage marker. Low can mean depletion. High needs context.
Serum iron: circulating iron at that moment. Useful, but fluctuates.
TIBC or transferrin: how much iron-binding capacity is available.
Transferrin saturation: one of the most useful screens for overload patterns.
CBC: hemoglobin, MCV, RDW, and anemia pattern.
hs-CRP: helps interpret ferritin as an inflammation marker.
Liver enzymes and metabolic context: ALT, AST, GGT, A1c, fasting insulin, lipids, alcohol, fatty liver risk.
HFE testing, when appropriate: especially with repeatedly high ferritin and transferrin saturation, family history, northern European ancestry, abnormal liver enzymes, diabetes, joint symptoms, or unexplained fatigue.
If the first panel looks strange, repeat it in a clean context when possible: no acute infection, no hard workout the day before, and ideally fasting in the morning. One odd lab is a clue. A repeated pattern is a case.
For iron deficiency in inflammatory conditions, the interpretation can get tricky. A Blood Advances review is a good reminder that inflammation can hide deficiency behind a ferritin that looks “normal.”
Translation: if someone tells you “your ferritin is normal” and nothing else was checked, you may not actually be done.
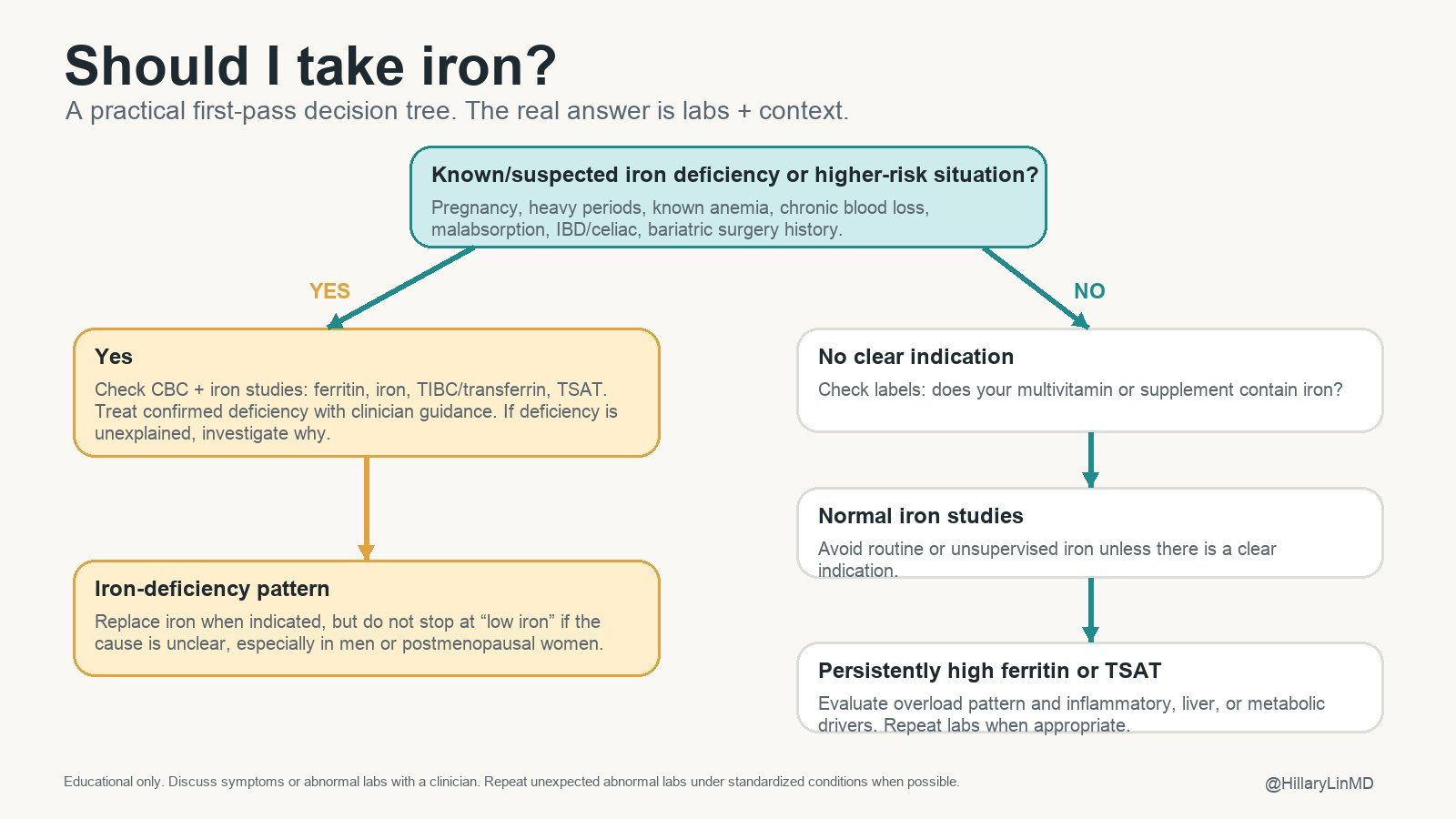
The iron decision tree. Treat confirmed deficiency when indicated, investigate unexplained deficiency, and avoid routine iron when labs and context do not support it.
Vitamin C is interesting again, but not a religion
I have historically been underwhelmed by most vitamin C takes.
Not because vitamin C is unimportant. It is essential. Severe deficiency gives you scurvy, which is quite a dramatic way for the body to ask for fruit.
The problem is the wellness narrative: take a lot, boost immunity, antioxidants, repeat forever.
The ACSL4 finding is better than that. It suggests vitamin C may interrupt part of the iron-lipid damage pathway upstream, instead of only mopping up free radicals afterward.
That does not mean more is always better.
Classic vitamin C pharmacokinetic data show that oral absorption drops as dose rises and plasma levels saturate. At higher doses, you excrete more.
My practical read:
Get vitamin C from food daily, not once a week in a guilt smoothie.
If your diet is inconsistent, a modest supplement can be reasonable.
Be cautious with chronic high doses if you have kidney stone history, advanced kidney disease, iron overload, or unclear iron status.
Do not treat a primate mechanism paper like a human dosing guideline.
Food anchors that actually work:
Kiwi
Citrus
Strawberries
Red bell pepper
Broccoli
Brussels sprouts
Guava, objectively elite fruit.
What I would actually do
1. Turn the bottle around
Check whether your multivitamin contains iron.
If you are a man or post-menopausal woman and your multivitamin contains iron, ask why. If the answer is “I have no idea,” that is not a medical indication.
2. Test before supplementing
Do not diagnose iron deficiency from fatigue alone.
Fatigue can be iron deficiency. It can also be sleep debt, thyroid disease, low B12, depression, overtraining, infection, poor nutrition, perimenopause, medication effects, or the fact that modern life is basically a browser with 47 tabs open.
Test.
3. Treat real deficiency
If you are deficient, treat it and look for the cause.
Heavy menstrual bleeding, pregnancy, GI blood loss, low intake, celiac disease, IBD, bariatric surgery, and chronic inflammation are different problems. Iron is treatment, but the “why” still matters.
4. Stop casual iron if you are replete
If your iron stores are adequate and you have no clear indication, I do not see a good reason to take supplemental iron.
A supplement without an indication is not prevention. It is an experiment you forgot you were running.
5. Use vitamin C intelligently
If you are plant-based or iron deficient, vitamin C with meals can improve non-heme iron absorption.
If you are iron-replete, vitamin C may still be useful for other reasons, but I would keep the dose boring and defensible unless there is a clear reason to do otherwise. Boring is underrated in supplement land.
6. Do not turn mechanism into certainty
Ferro-aging is compelling. Vitamin C is plausible. The primate data are worth attention.
But the human move today is simple: test iron properly, avoid unnecessary iron, and stop ignoring old nutrients just because they are not shiny.
The bigger picture
The point is not that iron is dangerous.
The point is fit.
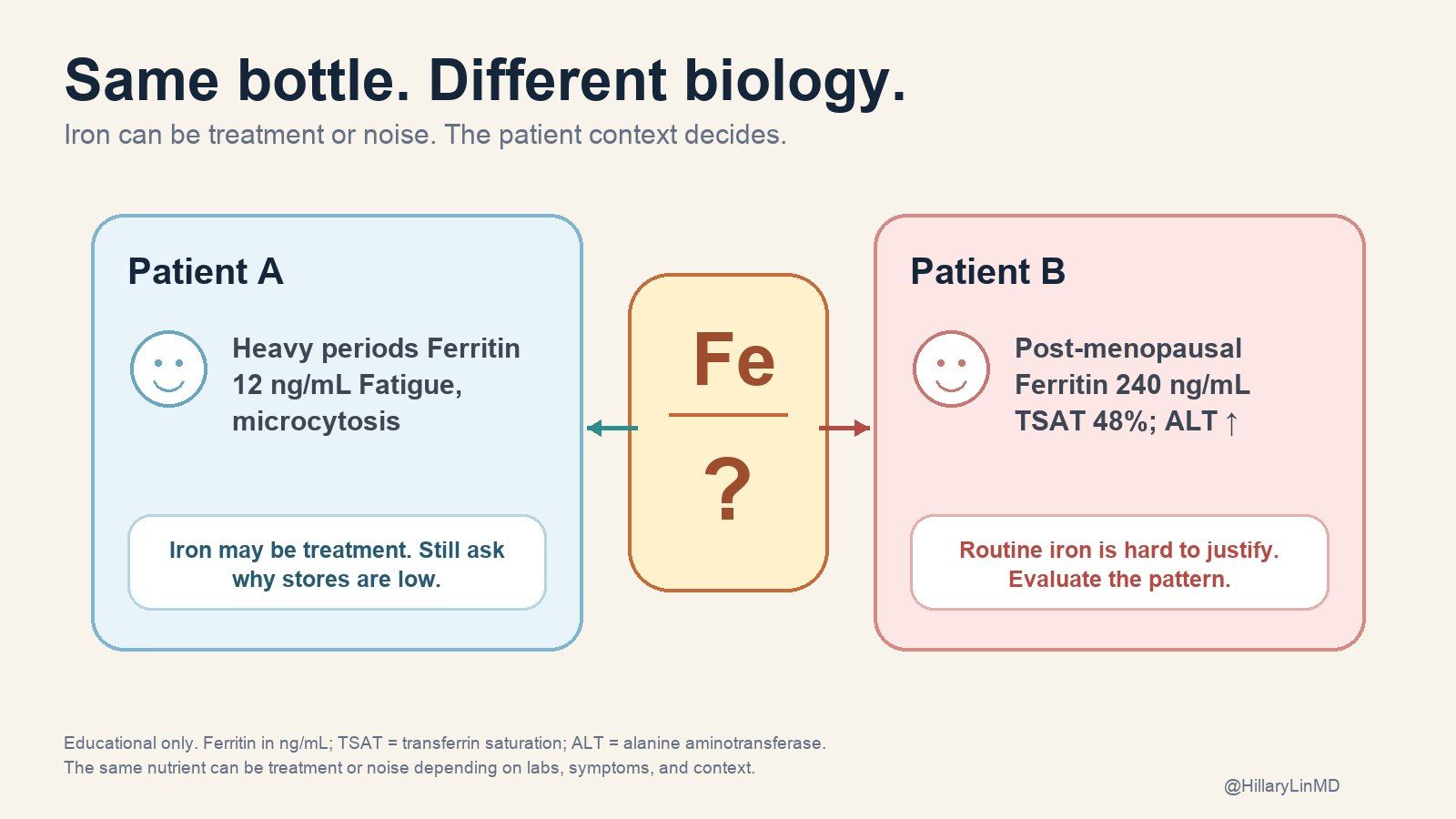
The same capsule can be treatment for one person and a bad idea for another. A 32-year-old with heavy periods and ferritin of 12 is not the same patient as a 62-year-old man with ferritin 240, transferrin saturation 48%, ALT elevation, and an iron-containing multivitamin. Same bottle. Different biology.
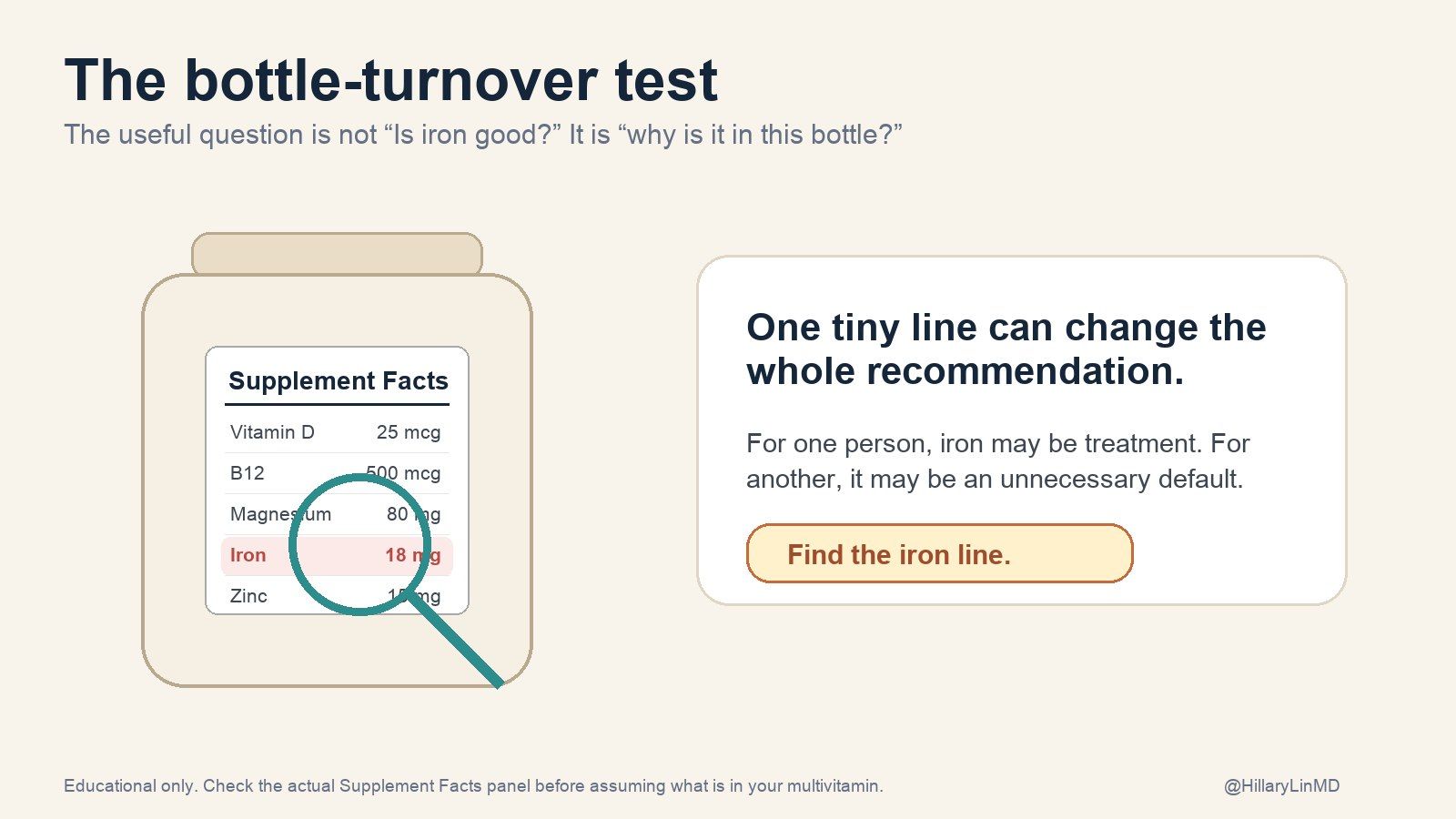
So here is the bottle-turnover test:
Pick up the supplement you take most often. Find the iron line.
If it contains iron, ask one question:
What lab result made this a good idea?
If you have an answer, great. If the answer is “I think it was just in there,” that is not a protocol. That is a default setting pretending to be medical care.
Forward this to one person who takes a multivitamin and has never read the iron line. Gentle chaos. Clinically useful.
Longevity quick hits
🧪 Plastic exposure can move fast. In the PERTH randomized trial, a 7-day low-plastic intervention lowered urinary mono-n-butyl phthalate, monobenzyl phthalate, and BPA. Not outcomes proof, but very actionable exposure data.
💉 GLP-1 weight loss still has a muscle problem. An Annals of Internal Medicine systematic review found muscle-related losses exceeded prespecified benchmarks in about two thirds of incretin-based interventions with body-composition reporting. GLP-1s may be longevity drugs, but only if patients do not lose the wrong tissue.
🧬 Metformin did not win the geroscience lottery. In METFORAGING, non-diabetic older adults with well-controlled HIV took metformin for 96 weeks. The primary epigenetic-age outcome was not significantly different. Useful pilot, not a victory lap.
🧠 Brain aging is not just personal discipline. A Nature Medicine exposome study linked physical, social, and sociopolitical exposures across 40 countries with accelerated aging signals. Prevention is biology plus environment, not just willpower with a wearable.
🍽️ Beta cells adapt until they cannot. A Nature Metabolism beta-cell methylation study suggests healthy beta cells remodel epigenetically with age, while type 2 diabetes may accelerate that adaptation toward failure. Metabolic disease is partly failed compensation over time.
From The Longevity Show
Navigating the Supplement Maze
I made this because patients keep bringing in supplement stacks that look thoughtful, expensive, and sometimes completely disconnected from their actual labs. We get into multivitamins, biohacking, testing, and the boring-but-useful question I wish more people asked: what problem is this supposed to solve?
If this issue made you turn over your multivitamin bottle, good.
That tiny Supplement Facts panel has started more useful medical conversations than several very expensive wellness panels I have seen.
Keep learning,
Hillary Lin, MD
Co-Founder & CEO, CareCore
Was this useful? Forward The Longevity Letter to someone who would benefit.
Want to turn your wellness brand into a full-service health destination? Learn about CareCore's platform or Get Started Here.
Where to find me
The Aging Code Summit, May 26-27, Mosesian Center for the Arts, Greater Boston. I’ll be on the clinician panel discussing how aging research translates into real interventions.
NYC Tech Week: “Sick Care Is Dead”, June 2, New York, NY. A panel on what actually comes after the old model. If you're in NYC and building in health, this is the room to be in.
Dry Eye Society of the Americas, July 10-11, 2026, NYC. Dry eyes are a growing problem and symptom of deeper issues tied to longevity. For clinicians, join us.
Science of Skin Summit, September 17-20, Austin, TX. I’m speaking twice: one session on AI in dermatology, one on skin and hair as windows into biological age. For clinicians.
Support us with your longevity purchases
🐟 Seatopia — sustainable, sashimi-grade seafood checked for microplastics and mercury. Code HILLARYLINMD for $20 off.
⏱️ Timeline — patented Urolithin A for scientifically proven mitochondrial support via mitophagy. Code CARECORE for 10% off.
🍺 ZBiotics — pro-longevity probiotics for when you do have a little fun. Code CARECORE for 10% off.
🧲 CoreViva — whole-body MRI screening for early disease detection. Code CARECORE for $200 off.
🧠 NeuroAgeTx — the most comprehensive brain aging package at up to 61% off for Longevity Letter readers.
🧬 GlycanAge — measures your immune system's biological age and recommends how to fix it.
Advanced diagnostics
Want to know your biological age? Check out our testing page for epigenetic age testing with physician consultation, including TruDiagnostic TruAge and SystemAge by Generation Lab.
Have a question or topic you want covered? Reply to this email.
Was this forwarded to you? Subscribe here to get The Longevity Letter in your inbox.
The Longevity Letter
A weekly read on tests, treatment, and claims.
New issues look at what the evidence supports, what is premature, and what to skip.